You might also like
- Association Between MRNA Expression of Aromatase 1Document8 pagesAssociation Between MRNA Expression of Aromatase 1Nenny Yoanitha DjalaNo ratings yet
- Palliative Care - Modul NennyDocument31 pagesPalliative Care - Modul NennyNenny Yoanitha DjalaNo ratings yet
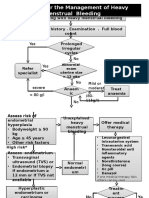
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- En Endometrial Cancer Guide For PatientsDocument30 pagesEn Endometrial Cancer Guide For PatientsNenny Yoanitha DjalaNo ratings yet
- Hypertensionin PregnancyDocument100 pagesHypertensionin Pregnancyricky hutagalungNo ratings yet
- Estimated Fetal Weight Formula GuideDocument5 pagesEstimated Fetal Weight Formula GuideNenny Yoanitha Djala100% (1)
- Night Shift Duty 11 FEBRUARIDocument2 pagesNight Shift Duty 11 FEBRUARINenny Yoanitha DjalaNo ratings yet
- AJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenDocument6 pagesAJOG 2008 - Amoxicillin Pharmacokinetics in Pregnant WomenNenny Yoanitha DjalaNo ratings yet
- Program Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Document1 pageProgram Kerja Gugus Kendali Mutu SMF Obstetri dan Ginekologi 2017-2018Nenny Yoanitha DjalaNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- American Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFDocument6 pagesAmerican Journal of Obstetrics and Gynecology Volume 207 Issue 3 2012 (Doi 10.1016/j.ajog.2012.07.031) McPherson, Jessica A. Odibo, Anthony O. Shanks, Anthony L. Ro - Impact of Chorionicity On R PDFNenny Yoanitha DjalaNo ratings yet
- Forceps Review in Modern Obstetric PracticeDocument5 pagesForceps Review in Modern Obstetric PracticeNenny Yoanitha DjalaNo ratings yet
- Strategi Bisnis KorporasiDocument41 pagesStrategi Bisnis KorporasiAliMu'minHarahapNo ratings yet
- Termination Pregnancy Report 18 May 2010Document45 pagesTermination Pregnancy Report 18 May 2010Nenny Yoanitha DjalaNo ratings yet
- Obstetrical Forceps - History Mystery and MoralityDocument16 pagesObstetrical Forceps - History Mystery and MoralityNenny Yoanitha DjalaNo ratings yet
- Medical Eligibility Criteria For Contraceptive Use Fifth Edition 2015Document14 pagesMedical Eligibility Criteria For Contraceptive Use Fifth Edition 2015agustinasntNo ratings yet
- How To Explore After Forceps ExtractionDocument7 pagesHow To Explore After Forceps ExtractionNenny Yoanitha DjalaNo ratings yet
- Anatomical Causes Bad Obstetric HistoryDocument3 pagesAnatomical Causes Bad Obstetric Historykyle31No ratings yet
- Fetal and Maternal Effects of Forceps and VacuumDocument4 pagesFetal and Maternal Effects of Forceps and VacuumNenny Yoanitha DjalaNo ratings yet
- Final Data 2011 PDFDocument90 pagesFinal Data 2011 PDFNenny Yoanitha DjalaNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Trali Dari Ats JournalDocument2 pagesTrali Dari Ats JournalNenny Yoanitha DjalaNo ratings yet
- Algorithm For The Management of Heavy Menstrual BleedingDocument2 pagesAlgorithm For The Management of Heavy Menstrual BleedingNenny Yoanitha DjalaNo ratings yet
- Cytomegalovirus Infection in Patients With Active InflammatoryDocument7 pagesCytomegalovirus Infection in Patients With Active InflammatoryNenny Yoanitha DjalaNo ratings yet
- Forceps ExtractionDocument49 pagesForceps ExtractionNenny Yoanitha DjalaNo ratings yet
- Genetic Study of TORCH Infections in Women With BOH PDFDocument6 pagesGenetic Study of TORCH Infections in Women With BOH PDFNenny Yoanitha DjalaNo ratings yet
- Reichman 2014Document5 pagesReichman 2014Nenny Yoanitha DjalaNo ratings yet
- Successful Pregnancy OutcomeDocument6 pagesSuccessful Pregnancy OutcomeNenny Yoanitha DjalaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 3rd Annual Radiology For Non-Radiologists (5-6 Oct 2019)Document2 pages3rd Annual Radiology For Non-Radiologists (5-6 Oct 2019)itnnetworkNo ratings yet
- General Pathology MCQDocument3 pagesGeneral Pathology MCQSooPl33% (3)
- Cephalometric Evaluation of GrowthDocument79 pagesCephalometric Evaluation of GrowthAhmedsy Ahmedsy AhmedsyNo ratings yet
- Surgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesDocument7 pagesSurgical Specimen Management: A Descriptive Study of 648 Adverse Events and Near MissesRubia Sari Mamanya HaristNo ratings yet
- Velammal VistDocument30 pagesVelammal VistpriyaNo ratings yet
- Notification Babu Jagjivan Ram Memorial Hospital SR Resident PostsDocument5 pagesNotification Babu Jagjivan Ram Memorial Hospital SR Resident PostsJeshiNo ratings yet
- 04.03-02 Endocrine IV - Uterine Pharmacology PDFDocument4 pages04.03-02 Endocrine IV - Uterine Pharmacology PDFMaikka IlaganNo ratings yet
- Gestational AgeDocument4 pagesGestational AgeNadya Nur AqilahNo ratings yet
- Placenta Previa MarginalDocument50 pagesPlacenta Previa MarginalMedy WedhanggaNo ratings yet
- Vandykediann ResumeDocument3 pagesVandykediann ResumeHARSHANo ratings yet
- BibliographyDocument21 pagesBibliographyapi-204960846No ratings yet
- Kangaroo Joey ManualDocument16 pagesKangaroo Joey ManualCarmen Leiva AsencioNo ratings yet
- Factors Affecting Utilization of Maternal Health CDocument8 pagesFactors Affecting Utilization of Maternal Health CYussufNo ratings yet
- Case presentation on short stature and pubertal delay in a 14-year-old maleDocument27 pagesCase presentation on short stature and pubertal delay in a 14-year-old maledidu91No ratings yet
- Live Before You DieDocument6 pagesLive Before You DieCharms CabauatanNo ratings yet
- Third Stage of Labour Lastt Last LastDocument30 pagesThird Stage of Labour Lastt Last LastAyanayuNo ratings yet
- CV Elective Program For International StudentsDocument5 pagesCV Elective Program For International StudentsYosafatPrasetyadiNo ratings yet
- ISICAM TimetableDocument8 pagesISICAM TimetableMichael SusantoNo ratings yet
- 2018 UNICEF Eswatini Neonatal GuidelinesDocument180 pages2018 UNICEF Eswatini Neonatal GuidelinesTrishenth FonsekaNo ratings yet
- Smart Solutions For OB/GYN: ACUSON X Family and ACUSON P Family Ultrasound SystemsDocument8 pagesSmart Solutions For OB/GYN: ACUSON X Family and ACUSON P Family Ultrasound SystemsPopescu ValiNo ratings yet
- Maquet LyraDocument12 pagesMaquet LyraMiguel YepesNo ratings yet
- Botiss Maxgraft Bonebuilder SurgicalGuideDocument11 pagesBotiss Maxgraft Bonebuilder SurgicalGuideDemmy WijayaNo ratings yet
- Periodontal FlapsDocument65 pagesPeriodontal FlapsSaleh AlsadiNo ratings yet
- KAREEN PRC FILE Corrected FinalDocument10 pagesKAREEN PRC FILE Corrected Finaljedkath2008No ratings yet
- Traumatic Diaphragmatic Hernia Anaesthetic ConsideDocument3 pagesTraumatic Diaphragmatic Hernia Anaesthetic ConsideHalim SudonoNo ratings yet
- Mccee QuestionsDocument69 pagesMccee QuestionsAndre R. Reynolds Anglin100% (3)
- Transcutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementDocument54 pagesTranscutaneous Electrical Nerve Stimulation (Tens) and Pain ManagementhashfiluthfihNo ratings yet
- 2017.104 - The - Leopold - Maneuver - PosterDocument1 page2017.104 - The - Leopold - Maneuver - PosterRey CelNo ratings yet
- Facial ContoursDocument20 pagesFacial Contourscmkflorida7011100% (1)
- Plan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Document7 pagesPlan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Rinor MujajNo ratings yet