You might also like
- ACLS Algorithms SlideDocument26 pagesACLS Algorithms SlidehrsoNo ratings yet
- ACLS Training - Most Important Points To RememberDocument5 pagesACLS Training - Most Important Points To RememberEman ElzeftawyNo ratings yet
- Normal Ranges Vital Signs 2017Document2 pagesNormal Ranges Vital Signs 2017Elvis Nguyen100% (1)
- REPORT Mandela Kibiriti's ACLS scoresDocument2 pagesREPORT Mandela Kibiriti's ACLS scoresMandela KibiritiNo ratings yet
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDocument8 pagesAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyNo ratings yet
- ACLS and PALS Certification Practice QuestionsDocument11 pagesACLS and PALS Certification Practice Questionsdyah rahayu hutamiNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahNo ratings yet
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDocument1 pageAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNo ratings yet
- Introd To ECG Code Blue Champs March 2019Document52 pagesIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- Acls MegacodeDocument8 pagesAcls Megacodes33d_destinyNo ratings yet
- PALS Precourse Self 2023Document9 pagesPALS Precourse Self 2023Airene SibleNo ratings yet
- ACLS QuizletDocument7 pagesACLS Quizletek.9006001No ratings yet
- ACLS Official GuideDocument11 pagesACLS Official GuideICU RSPGNo ratings yet
- Aha Acls Prep Packet 2020Document69 pagesAha Acls Prep Packet 2020VP The Hacker100% (2)
- 15 Item ACLS Drill With RationaleDocument12 pages15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- Nursing Responsibilities in Handling AntibioticsDocument4 pagesNursing Responsibilities in Handling Antibioticsrichardmd20% (1)
- ACLS Algorithms (2011)Document6 pagesACLS Algorithms (2011)senbonsakuraNo ratings yet
- ACLS DrugDocument7 pagesACLS DrugPhongsatorn Thunin100% (1)
- ACLS Skills ChecklistDocument2 pagesACLS Skills ChecklistKary ParraNo ratings yet
- CPR Class QuestionnaireDocument4 pagesCPR Class QuestionnaireParikshit PekhaleNo ratings yet
- PALS Precourse Self-AssessmentDocument2 pagesPALS Precourse Self-AssessmentGabriel Del RosarioNo ratings yet
- ACLS Review Guide for Cardiac Arrest Scenarios and TreatmentDocument29 pagesACLS Review Guide for Cardiac Arrest Scenarios and TreatmentJB Reyes100% (2)
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- Code Blue MedsDocument35 pagesCode Blue Medssbjon984924100% (1)
- Emergency Cart FinalDocument17 pagesEmergency Cart FinalWoo Bin100% (1)
- ALS Manual PDFDocument74 pagesALS Manual PDFBlack Owell100% (1)
- TestDocument11 pagesTestzenagit123456100% (1)
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- Hospital and Critical CareDocument16 pagesHospital and Critical CareMarivy GalonNo ratings yet
- ACLS PrecourseAssessmentDocument19 pagesACLS PrecourseAssessmentRaiedKhaled100% (1)
- ACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONDocument3 pagesACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONaditNo ratings yet
- ACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsDocument10 pagesACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsChintami Octavia100% (1)
- BLS MCQDocument8 pagesBLS MCQAmit BhowmikNo ratings yet
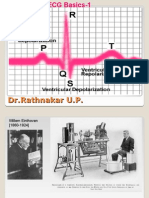
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- American Heart Association Acls Post Test AnswersDocument4 pagesAmerican Heart Association Acls Post Test AnswersArun Jude Alphonse0% (9)
- Bls Question 1Document7 pagesBls Question 1balderas135384No ratings yet
- BLS ALGORITHM As of February 2023Document2 pagesBLS ALGORITHM As of February 2023Mark Jason Rodriguez, RNNo ratings yet
- Soalan MCQ Acls Fit Set BDocument3 pagesSoalan MCQ Acls Fit Set BAnonymous 89ilBIGhrmNo ratings yet
- ACLS Simulation ScenariosDocument14 pagesACLS Simulation ScenariosVanessa HermioneNo ratings yet
- ACLS Written 2006 Precourse Self AssessmentDocument14 pagesACLS Written 2006 Precourse Self AssessmentmonickamsNo ratings yet
- Pediatric Cardiac Arrest and Bradycardia AlgorithmsDocument6 pagesPediatric Cardiac Arrest and Bradycardia AlgorithmsandiyanimalikNo ratings yet
- Aha Acls Algorithms 2010Document13 pagesAha Acls Algorithms 2010Imania AssagafNo ratings yet
- 15 item ACLS Drill ReviewDocument4 pages15 item ACLS Drill ReviewVal SolidumNo ratings yet
- ACLS Pharmacology Pretest Question Answers PDF (SET-2)Document9 pagesACLS Pharmacology Pretest Question Answers PDF (SET-2)김민길100% (1)
- Cardiac Arrest Drugs & ProceduresDocument8 pagesCardiac Arrest Drugs & ProceduresAstri Adel BudiarsoNo ratings yet
- Cals ReviewbjvjvjDocument14 pagesCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- AclsDocument21 pagesAclsMelvin Sierra TejedaNo ratings yet
- Mastering Electocardiograms - Honda-2Document3 pagesMastering Electocardiograms - Honda-2Christian MacielNo ratings yet
- ICU Guideline: Temporary Cardiac PacingDocument8 pagesICU Guideline: Temporary Cardiac PacingistiNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- EKG Rhythms: SVT, Atrial Fibrillation, AV Blocks (39Document10 pagesEKG Rhythms: SVT, Atrial Fibrillation, AV Blocks (39Saidel ElizondoNo ratings yet
- Medsurg 3 Exam 1Document55 pagesMedsurg 3 Exam 1Melissa Blanco100% (1)
- ACLS Notes: Cardiac Emergencies GuideDocument6 pagesACLS Notes: Cardiac Emergencies GuideHalina Miranda MirandaNo ratings yet
- Oral Board Exam AudioDocument64 pagesOral Board Exam AudioMahjong SirenNo ratings yet
- Manoj Patil (12) Vishal WaghDocument3 pagesManoj Patil (12) Vishal WaghSeno SenyNo ratings yet
- Ovarian Cysts Overview: Menstrual Cycle Pregnancy UltrasoundDocument13 pagesOvarian Cysts Overview: Menstrual Cycle Pregnancy Ultrasoundzerocoolz123No ratings yet
- Question Clinical Anatomy of The Visual System FFXDocument4 pagesQuestion Clinical Anatomy of The Visual System FFXaditya febriansyahNo ratings yet
- HOME vs HOSPITALDocument19 pagesHOME vs HOSPITALdevNo ratings yet
- 2021 GS Lesson 1. DesmurgyDocument39 pages2021 GS Lesson 1. DesmurgyearNo ratings yet
- Surgical Equipment ListDocument6 pagesSurgical Equipment Listbnbmiller3100% (4)
- Bladder IrrigationDocument19 pagesBladder IrrigationDwight Kristian CruzNo ratings yet
- Oral Anatomy ReviewerDocument57 pagesOral Anatomy ReviewerJEVELYN D. TUMBAGANo ratings yet
- Anatomy of the Pelvis & PerineumDocument162 pagesAnatomy of the Pelvis & PerineumKolawole Adesina KehindeNo ratings yet
- Detailed Lesson Plan in Health FinalDocument8 pagesDetailed Lesson Plan in Health FinalRochedel Asuncion100% (1)
- Issam Abouliatim, MDDocument19 pagesIssam Abouliatim, MDNaser Hamdi ZalloumNo ratings yet
- Chapter 6 Test ControlDocument7 pagesChapter 6 Test ControlSheikhNo ratings yet
- Well-Lead-Catalogue 2021 PDFDocument62 pagesWell-Lead-Catalogue 2021 PDFDaniel Algarañaz LoboNo ratings yet
- Coronoid Process AnatomyDocument7 pagesCoronoid Process AnatomyZulhajja Nur08No ratings yet
- Manual For EndosDocument19 pagesManual For EndosVarsha MalikNo ratings yet
- Thomas J. Fogarty MD, Amitava Biswas MD (Auth.), Thomas J. Fogarty, Rodney A. White (Eds.) - Peripheral Endovascular Interventions-Springer-Verlag New York (2010)Document509 pagesThomas J. Fogarty MD, Amitava Biswas MD (Auth.), Thomas J. Fogarty, Rodney A. White (Eds.) - Peripheral Endovascular Interventions-Springer-Verlag New York (2010)Mircea Eugen MutuNo ratings yet
- Acute ComaDocument16 pagesAcute ComaDean AccountNo ratings yet
- Large External Fixator.: Allows Modularity in All Three PlanesDocument6 pagesLarge External Fixator.: Allows Modularity in All Three PlanesRazmig BedrosianNo ratings yet
- Aortic DissectionDocument49 pagesAortic DissectionAnonymous ZUaUz1wwNo ratings yet
- Contoh Makalah BioetikDocument35 pagesContoh Makalah Bioetiki.melahdaNo ratings yet
- Induksi Persalinan MetodeDocument20 pagesInduksi Persalinan MetodenilajmasptnaNo ratings yet
- BJAS-Volume 3-Issue 1 - Page 11-16Document6 pagesBJAS-Volume 3-Issue 1 - Page 11-16rakaNo ratings yet
- 3i CatalogDocument79 pages3i CatalogJulie HollowayNo ratings yet
- Basic VitrectomyDocument24 pagesBasic Vitrectomykomitemedik.rsudsdaNo ratings yet
- Management of Liver Trauma in Adults: Nasim Ahmed, Jerome J VernickDocument7 pagesManagement of Liver Trauma in Adults: Nasim Ahmed, Jerome J VernickwiraNo ratings yet
- Complications of Orthognathic SurgeryDocument39 pagesComplications of Orthognathic SurgeryAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- The Laryngeal Mask Airway: Technical Guidelines and Use in Special SituationsDocument10 pagesThe Laryngeal Mask Airway: Technical Guidelines and Use in Special Situationsjangkrik21No ratings yet
- BHRC Rates 01.04Document87 pagesBHRC Rates 01.04nishant00032No ratings yet
- Lateral Tendon Disorders Peroneal Tendinopathy Differential DiagnosisDocument5 pagesLateral Tendon Disorders Peroneal Tendinopathy Differential Diagnosischu_chiang_3No ratings yet