You might also like
- Syllabus Phar 6205Document6 pagesSyllabus Phar 6205Alex PiecesNo ratings yet
- Drug and Alcohol Psychosocial Interventions Professional Practice GuidelinesDocument94 pagesDrug and Alcohol Psychosocial Interventions Professional Practice GuidelinesAlex PiecesNo ratings yet
- There is now widespread recognition that Australia’s population is ageing and that this has important implications for the national economy and society. Despite this there is considerable misunderstanding of the nature, scale, location and implications of population ageing in Australia. This is even the case in the aged care sector which is to be so crucially impacted by the ageing of the population. The aim of this policy brief and the following two briefs (March and April, 2014) is to summarise the basic dimensions of the growth of Australia’s older population over the next two decades. The note will use the most recent Australian Bureau of Statistics (ABS, 2013a) population projections. It must be stressed, however, that for older populations there is no element of ‘crystal ball gazing’ in these projections. There is a very high degree of certainty around them and they can be used with a high degree of confidence. This is because Australia’s older population of the 2020s and 2Document7 pagesThere is now widespread recognition that Australia’s population is ageing and that this has important implications for the national economy and society. Despite this there is considerable misunderstanding of the nature, scale, location and implications of population ageing in Australia. This is even the case in the aged care sector which is to be so crucially impacted by the ageing of the population. The aim of this policy brief and the following two briefs (March and April, 2014) is to summarise the basic dimensions of the growth of Australia’s older population over the next two decades. The note will use the most recent Australian Bureau of Statistics (ABS, 2013a) population projections. It must be stressed, however, that for older populations there is no element of ‘crystal ball gazing’ in these projections. There is a very high degree of certainty around them and they can be used with a high degree of confidence. This is because Australia’s older population of the 2020s and 2Alex PiecesNo ratings yet
- Sub Skin Cancer Inquiry 21 March 2014Document23 pagesSub Skin Cancer Inquiry 21 March 2014Alex PiecesNo ratings yet
- Cosa Submission Towards A National Cancer Research Plan April2012Document12 pagesCosa Submission Towards A National Cancer Research Plan April2012Alex PiecesNo ratings yet
- Medicare Exemption PDFDocument2 pagesMedicare Exemption PDFAlex PiecesNo ratings yet
- Bronchospasm Anesthesia PDFDocument6 pagesBronchospasm Anesthesia PDFAlex PiecesNo ratings yet
- Melanoma AustraliaDocument56 pagesMelanoma AustraliaAlex Pieces100% (1)
- CancerWorkYou NSW LoDocument60 pagesCancerWorkYou NSW LoAlex PiecesNo ratings yet
- CancerWorkYou NSW LoDocument60 pagesCancerWorkYou NSW LoAlex PiecesNo ratings yet
- Fish Omega3 Fatty Acids and Cancer Position StatementDocument13 pagesFish Omega3 Fatty Acids and Cancer Position StatementAlex PiecesNo ratings yet
- AYA Cancer Care Pathway Dec 2014Document146 pagesAYA Cancer Care Pathway Dec 2014Alex PiecesNo ratings yet
- PreCommencement Medical History Form v2Document3 pagesPreCommencement Medical History Form v2Alex PiecesNo ratings yet
- ATAC Fact SheetDocument3 pagesATAC Fact SheetAlex PiecesNo ratings yet
- List of Successful GrantsDocument3 pagesList of Successful GrantsAlex PiecesNo ratings yet
- Lewin Application - TenancyDocument3 pagesLewin Application - TenancyAlex PiecesNo ratings yet
- CRLF Maximising The Impact of Cancer Research Funding in AustraliaDocument29 pagesCRLF Maximising The Impact of Cancer Research Funding in AustraliaAlex PiecesNo ratings yet
- CA Audit Report FinalDocument167 pagesCA Audit Report FinalAlex PiecesNo ratings yet
- Gen F QLD Stat DecDocument20 pagesGen F QLD Stat DecAlex PiecesNo ratings yet
- NSW Health Records Policy SummaryDocument21 pagesNSW Health Records Policy SummaryhopeloltestscribdNo ratings yet
- Mediserve QLD Nurse Reg (Print)Document11 pagesMediserve QLD Nurse Reg (Print)Alex PiecesNo ratings yet
- Nursing Shift Break AgreementDocument1 pageNursing Shift Break AgreementAlex PiecesNo ratings yet
- Gen F QLD Stat DecDocument1 pageGen F QLD Stat DecAlex PiecesNo ratings yet
- Cprf-022 Precom Employee v5 Not Plumber Child CareDocument2 pagesCprf-022 Precom Employee v5 Not Plumber Child CareAlex PiecesNo ratings yet
- Problems That Occur Within Pacu IncludeDocument3 pagesProblems That Occur Within Pacu IncludeAlex PiecesNo ratings yet
- ATO New Choice Form (Only Print Pages 5-7)Document7 pagesATO New Choice Form (Only Print Pages 5-7)Alex PiecesNo ratings yet
- Perioperative Skills ChecklistDocument61 pagesPerioperative Skills ChecklistAlex PiecesNo ratings yet
- Problems That Occur Within Pacu IncludeDocument1 pageProblems That Occur Within Pacu IncludeAlex PiecesNo ratings yet
- PerioperativeSkillsChecklist PDFDocument13 pagesPerioperativeSkillsChecklist PDFAlex PiecesNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Naruto ThemeDocument8 pagesNaruto ThemeFritzie AileNo ratings yet
- RET (Mains) 2024 - JamshedprDocument2 pagesRET (Mains) 2024 - Jamshedpraarushitv.11No ratings yet
- SM 3Document14 pagesSM 3Nuty IonutNo ratings yet
- Genshin Best Character Ranking Calculator All Character Sorter Genshin Impact - GameWith PDFDocument1 pageGenshin Best Character Ranking Calculator All Character Sorter Genshin Impact - GameWith PDFparitamehta2804No ratings yet
- Friction Clutches 2020 CompressedDocument14 pagesFriction Clutches 2020 Compressedfikadu435No ratings yet
- ChordsDocument2 pagesChordsMadison ColeNo ratings yet
- Tencate Ms Pro Product LeafletDocument2 pagesTencate Ms Pro Product Leafletamee101296No ratings yet
- Idc4 Inglese v2Document8 pagesIdc4 Inglese v2Matt MarkNo ratings yet
- MembersListVIIthAssembly 3Document1 pageMembersListVIIthAssembly 3lakshayNo ratings yet
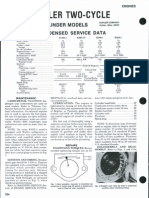
- One Cylinder ModelsDocument4 pagesOne Cylinder ModelsPaul MartinNo ratings yet
- sph4u momentum and energy exam review solutionsDocument7 pagessph4u momentum and energy exam review solutionsevanjohnstonespamNo ratings yet
- Xray t2r Pro Asphalt Rubber Spec Basic Setup SheetDocument1 pageXray t2r Pro Asphalt Rubber Spec Basic Setup Sheeteric hipolNo ratings yet
- Is golf an Olympic sport? Why it took so long to become oneDocument3 pagesIs golf an Olympic sport? Why it took so long to become oneMumtahina OishyNo ratings yet
- Distribuidores de Perfumes Originales al Por MayorDocument97 pagesDistribuidores de Perfumes Originales al Por MayorChristian Arias VeraNo ratings yet
- Modern Chess Strategy PDFDocument162 pagesModern Chess Strategy PDFSoham Saha100% (1)
- MAPEH Score Analysis for Grade 10Document3 pagesMAPEH Score Analysis for Grade 10Rodolfo Esmejarda Laycano Jr.No ratings yet
- EliteDocument3 pagesEliteSajjan JaiswalNo ratings yet
- Race 1: 1200Mts Time:1.15Pm 3yrsm Astro - Trainer-Jky C (3yrsm) +1200Document3 pagesRace 1: 1200Mts Time:1.15Pm 3yrsm Astro - Trainer-Jky C (3yrsm) +1200vv0% (1)
- August - Livshitz - Test Your Chess IQ. Tom 3. GM Challenge (1993)Document114 pagesAugust - Livshitz - Test Your Chess IQ. Tom 3. GM Challenge (1993)Tapculescu Marius67% (6)
- Gaslands - Rule of Carnage - Issue 1.0Document16 pagesGaslands - Rule of Carnage - Issue 1.0petri.ruotanen6205100% (2)
- Relationship Between Players Perfomance and SalaryDocument19 pagesRelationship Between Players Perfomance and SalaryyuliNo ratings yet
- CAB Door Components GuideDocument6 pagesCAB Door Components GuideSIA Stats RENTNo ratings yet
- Trago-10EM ETMDocument237 pagesTrago-10EM ETMHoàng VũNo ratings yet
- 2lt Arun Khetrapal, PVCDocument2 pages2lt Arun Khetrapal, PVCManish Mann IndoriaNo ratings yet
- Chin Up Bar Instructions PDFDocument1 pageChin Up Bar Instructions PDFHazwan ChuckNo ratings yet
- Activity On Arrow ExampleDocument2 pagesActivity On Arrow ExampleFernandoNo ratings yet
- 2018 - NHRA - Rulebook - Gen. Regs PDFDocument47 pages2018 - NHRA - Rulebook - Gen. Regs PDFahutchison5197No ratings yet
- Football Trading Compound Plan CalculatorDocument13 pagesFootball Trading Compound Plan CalculatorRaph SunNo ratings yet