You might also like
- Cmped 9 2015 067 PDFDocument6 pagesCmped 9 2015 067 PDFSarah Martinauli HarahapNo ratings yet
- Jos 16 27Document9 pagesJos 16 27Sarah Martinauli HarahapNo ratings yet
- JournalDocument7 pagesJournalSarah Martinauli HarahapNo ratings yet
- 2015 Article 353 PDFDocument7 pages2015 Article 353 PDFSarah Martinauli HarahapNo ratings yet
- Neurology JournalDocument7 pagesNeurology JournalSarah Martinauli HarahapNo ratings yet
- Stroke Journal 2015Document9 pagesStroke Journal 2015Sarah Martinauli HarahapNo ratings yet
- NeurologyDocument10 pagesNeurologySarah Martinauli HarahapNo ratings yet
- Jos 17 101 PDFDocument10 pagesJos 17 101 PDFSarah Martinauli HarahapNo ratings yet
- Jos 17 3 282Document23 pagesJos 17 3 282Sarah Martinauli HarahapNo ratings yet
- Smoking Is Not A Good Prognostic Factor Following First Ever Acute Ischemic StrokeDocument15 pagesSmoking Is Not A Good Prognostic Factor Following First Ever Acute Ischemic StrokeMuhammad Ilham FarizNo ratings yet
- The Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisDocument23 pagesThe Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-AnalysisSarah Martinauli HarahapNo ratings yet
- Journal AnakDocument6 pagesJournal AnakSarah Martinauli HarahapNo ratings yet
- Neurology JournalDocument7 pagesNeurology JournalSarah Martinauli HarahapNo ratings yet
- Clinical Study: Effects of A New Patient Safety-Driven Oxytocin Dosing Protocol On Postpartum HemorrhageDocument5 pagesClinical Study: Effects of A New Patient Safety-Driven Oxytocin Dosing Protocol On Postpartum HemorrhageRatih Kusuma DewiNo ratings yet
- Sleep Duration and Risk of Fatal and Nonfatal StrokeDocument10 pagesSleep Duration and Risk of Fatal and Nonfatal StrokemuhamadmukhlisNo ratings yet
- Pediatric Journal 5Document7 pagesPediatric Journal 5Sarah Martinauli HarahapNo ratings yet
- Pediatric Journal 6Document5 pagesPediatric Journal 6Sarah Martinauli HarahapNo ratings yet
- Pediatric Journal 6Document8 pagesPediatric Journal 6Sarah Martinauli HarahapNo ratings yet
- Bubble Nasal CPAPDocument9 pagesBubble Nasal CPAPHaniNo ratings yet
- Neurology Journal 8Document7 pagesNeurology Journal 8Sarah Martinauli HarahapNo ratings yet
- Pediatric Journal 3Document10 pagesPediatric Journal 3Sarah Martinauli HarahapNo ratings yet
- Pediatric Journal 2Document4 pagesPediatric Journal 2Sarah Martinauli HarahapNo ratings yet
- Pediatric JournalDocument5 pagesPediatric JournalSarah Martinauli HarahapNo ratings yet
- Jos 16 27Document9 pagesJos 16 27Sarah Martinauli HarahapNo ratings yet
- Journal StrokeDocument12 pagesJournal StrokeSarah Martinauli HarahapNo ratings yet
- Clinical Study: Sex, Diastolic Blood Pressure, and Outcome After Thrombolysis For Ischemic StrokeDocument8 pagesClinical Study: Sex, Diastolic Blood Pressure, and Outcome After Thrombolysis For Ischemic StrokeSarah Martinauli HarahapNo ratings yet
- Stroke Journal 2015Document9 pagesStroke Journal 2015Sarah Martinauli HarahapNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- L-1 Linear Algebra Howard Anton Lectures Slides For StudentDocument19 pagesL-1 Linear Algebra Howard Anton Lectures Slides For StudentHasnain AbbasiNo ratings yet
- 1.1 Introduction To Networks - Networks Affect Our LivesDocument2 pages1.1 Introduction To Networks - Networks Affect Our LivesCristian MoralesNo ratings yet
- Debentures Issued Are SecuritiesDocument8 pagesDebentures Issued Are Securitiesarthimalla priyankaNo ratings yet
- BUSINESS FINANCE - Activity 2Document3 pagesBUSINESS FINANCE - Activity 2Airish PascualNo ratings yet
- Welding MapDocument5 pagesWelding MapDjuangNo ratings yet
- 3838 Chandra Dev Gurung BSBADM502 Assessment 2 ProjectDocument13 pages3838 Chandra Dev Gurung BSBADM502 Assessment 2 Projectxadow sahNo ratings yet
- Legal Techniques (2nd Set)Document152 pagesLegal Techniques (2nd Set)Karl Marxcuz ReyesNo ratings yet
- E-TON - Vector ST 250Document87 pagesE-TON - Vector ST 250mariusgrosyNo ratings yet
- Calc Fields Networking and Sharing: Welcome ToDocument42 pagesCalc Fields Networking and Sharing: Welcome Toprashant adhikariNo ratings yet
- Part I-Final Report On Soil InvestigationDocument16 pagesPart I-Final Report On Soil InvestigationmangjuhaiNo ratings yet
- HI - 93703 Manual TurbidimetroDocument13 pagesHI - 93703 Manual Turbidimetrojesica31No ratings yet
- The Human Resource Department of GIK InstituteDocument1 pageThe Human Resource Department of GIK InstitutexandercageNo ratings yet
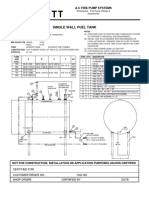
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsDocument1 pageSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoNo ratings yet
- Berry B Brey Part IDocument49 pagesBerry B Brey Part Ikalpesh_chandakNo ratings yet
- Chapter 3: Elements of Demand and SupplyDocument19 pagesChapter 3: Elements of Demand and SupplySerrano EUNo ratings yet
- 3DS MAX SYLLABUSDocument8 pages3DS MAX SYLLABUSKannan RajaNo ratings yet
- Leases 2Document3 pagesLeases 2John Patrick Lazaro Andres100% (1)
- Resume Ajeet KumarDocument2 pagesResume Ajeet KumarEr Suraj KumarNo ratings yet
- Meanwhile Elsewhere - Lizzie Le Blond.1pdfDocument1 pageMeanwhile Elsewhere - Lizzie Le Blond.1pdftheyomangamingNo ratings yet
- 7458-PM Putting The Pieces TogetherDocument11 pages7458-PM Putting The Pieces Togethermello06No ratings yet
- Sav 5446Document21 pagesSav 5446Michael100% (2)
- Abb Drives: User'S Manual Flashdrop Mfdt-01Document62 pagesAbb Drives: User'S Manual Flashdrop Mfdt-01Сергей СалтыковNo ratings yet
- Magnetism 02Document10 pagesMagnetism 02Niharika DeNo ratings yet
- Emperger's pioneering composite columnsDocument11 pagesEmperger's pioneering composite columnsDishant PrajapatiNo ratings yet
- Chapter 6: Structured Query Language (SQL) : Customer Custid Custname OccupationDocument16 pagesChapter 6: Structured Query Language (SQL) : Customer Custid Custname OccupationSarmila MahendranNo ratings yet
- Analytical DataDocument176 pagesAnalytical DataAsep KusnaliNo ratings yet
- Week 3 SEED in Role ActivityDocument2 pagesWeek 3 SEED in Role ActivityPrince DenhaagNo ratings yet
- Portable dual-input thermometer with RS232 connectivityDocument2 pagesPortable dual-input thermometer with RS232 connectivityTaha OpedNo ratings yet
- Developing a Positive HR ClimateDocument15 pagesDeveloping a Positive HR ClimateDrPurnima SharmaNo ratings yet
- Top Brand Story Bar Supervisor Jobs Chennai Apply Now Latest Fresher Experienced Bar Supervisor Jobs in Various Location July 18 2021Document1 pageTop Brand Story Bar Supervisor Jobs Chennai Apply Now Latest Fresher Experienced Bar Supervisor Jobs in Various Location July 18 2021Surya JamesNo ratings yet