You might also like
- Health Care Reform Act: Critical Tax and Insurance RamificationsFrom EverandHealth Care Reform Act: Critical Tax and Insurance RamificationsNo ratings yet
- PhilHealth Member Registration Form (PMRF)Document2 pagesPhilHealth Member Registration Form (PMRF)Vinson Gabato78% (9)
- (176736967) PMRF - RevisedDocument3 pages(176736967) PMRF - Revisedanon_902897556No ratings yet
- Philippine Health Insurance Corporation: Part I - Member InformationDocument1 pagePhilippine Health Insurance Corporation: Part I - Member InformationJANENo ratings yet
- Philippine Health Insurance Corporation: Part I - Member InformationDocument1 pagePhilippine Health Insurance Corporation: Part I - Member InformationjhunNo ratings yet
- Philhealth ClaimForm1 SignedDocument1 pagePhilhealth ClaimForm1 Signedjobelyn calaudNo ratings yet
- CF1 JabasDocument1 pageCF1 JabasqarlbalongNo ratings yet
- Philippine Health Insurance Corporation: Part I - Member InformationDocument1 pagePhilippine Health Insurance Corporation: Part I - Member InformationSnyrah AmbagNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersmikeeNo ratings yet
- Important RemindersDocument4 pagesImportant Remindersselvi agapitoNo ratings yet
- PDFDocument4 pagesPDFMaeralin Rose SagunNo ratings yet
- Sido Benita Chomacog 0 5 1 1 1 9 5 3 X: Poblacion Mankayan Benguet PhilippinesDocument1 pageSido Benita Chomacog 0 5 1 1 1 9 5 3 X: Poblacion Mankayan Benguet PhilippinesPrinston Del CampoNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersMoii Bautista CruzNo ratings yet
- Philhealth FormDocument2 pagesPhilhealth FormBuenavista Mae BautistaNo ratings yet
- Important RemindersDocument4 pagesImportant Remindersjm sausaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersLourd Juan Artuz MustafaNo ratings yet
- Important RemindersDocument16 pagesImportant RemindersMichael KitNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersJamieNo ratings yet
- File 9210Document8 pagesFile 9210JustaNo ratings yet
- Important RemindersDocument2 pagesImportant Remindersasdfjkl asddfNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersLyrics KingNo ratings yet
- Revenue Department, Govt. of NCT of Delhi Application Form For Other Backward ClassesDocument5 pagesRevenue Department, Govt. of NCT of Delhi Application Form For Other Backward ClassesSurinder VermaNo ratings yet
- Courtesy Lane Passport Application Form FillableDocument1 pageCourtesy Lane Passport Application Form Fillabledhie bumNo ratings yet
- Courtesy Lane Passport Application Form FillableDocument1 pageCourtesy Lane Passport Application Form Fillable9cwkwgccdjNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersKyndelle FajardoNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersKyndelle FajardoNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersTan TanNo ratings yet
- To ApplyDocument3 pagesTo ApplyElbert MagdoboyNo ratings yet
- 1 PDFDocument4 pages1 PDFSonny LardizábalNo ratings yet
- Passport Form A4Document2 pagesPassport Form A4RaquelNo ratings yet
- Form Ssa 454 BK FREEDocument14 pagesForm Ssa 454 BK FREEDicky keyNo ratings yet
- PDR 010713 PDFDocument1 pagePDR 010713 PDFFatima Qaushar ManamNo ratings yet
- Important RemindersDocument8 pagesImportant RemindersNewton AniguidNo ratings yet
- Important RemindersDocument2 pagesImportant Remindersroldan figuracionNo ratings yet
- If You Need Help Reading or Completing This Document or Need Help Communicating With Us, Ask Us orDocument19 pagesIf You Need Help Reading or Completing This Document or Need Help Communicating With Us, Ask Us ordavid rawlinsNo ratings yet
- PDFDocument4 pagesPDFIrish YongqueNo ratings yet
- 2018 Claim Signature FormDocument1 page2018 Claim Signature FormLorence VillaceranNo ratings yet
- Ssa 7163aDocument4 pagesSsa 7163ahoneyjam89No ratings yet
- Form SSA-3368-BKDocument14 pagesForm SSA-3368-BKMathis & MathisNo ratings yet
- 7 PDFDocument11 pages7 PDFArun SarkarNo ratings yet
- Member's Data Form (MDF, Hqp-pff-039, V04.1)Document5 pagesMember's Data Form (MDF, Hqp-pff-039, V04.1)Ron Villanueva0% (1)
- Important RemindersDocument4 pagesImportant Reminderskathlyn labradoNo ratings yet
- SAM-01 Client Application (3-10)Document1 pageSAM-01 Client Application (3-10)sandyolkowskiNo ratings yet
- Candidate QuestionnaireDocument6 pagesCandidate QuestionnairemaecelinocejaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersM IC M ICNo ratings yet
- Ssa 3368Document14 pagesSsa 3368JonOstiguyNo ratings yet
- ACFrOgAy2bR9GW6wnfl1fNzMKQcds XdQcim swMAKvXODLVz7iPyaO7ri12KfE5k6Qq5y8Hl0SDk386p1MLUBGYy5KKP5oABkUFIQXcZpL8z1O - 6Pq0MjB1AiFfOmU PDFDocument4 pagesACFrOgAy2bR9GW6wnfl1fNzMKQcds XdQcim swMAKvXODLVz7iPyaO7ri12KfE5k6Qq5y8Hl0SDk386p1MLUBGYy5KKP5oABkUFIQXcZpL8z1O - 6Pq0MjB1AiFfOmU PDFDeoo TriNo ratings yet
- English 13-14 App and LTRDocument5 pagesEnglish 13-14 App and LTRapi-259143520No ratings yet
- Important RemindersDocument4 pagesImportant RemindersJane Maranguit GonzalesNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersAldrin Palma AyalinNo ratings yet
- Asmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFDocument19 pagesAsmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFCardioTCSNo ratings yet
- ClaimSignatureForm 2018.1Document1 pageClaimSignatureForm 2018.1Lea MateoNo ratings yet
- SportsDocument4 pagesSportsWinty BandalNo ratings yet
- PLEASES Bora Nov 152022 JNEB INVITE With FormsDocument6 pagesPLEASES Bora Nov 152022 JNEB INVITE With Formshacketterz30No ratings yet
- Federal Benefits for Veterans, Dependents, and Survivors: Updated EditionFrom EverandFederal Benefits for Veterans, Dependents, and Survivors: Updated EditionRating: 5 out of 5 stars5/5 (1)
- Social Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceFrom EverandSocial Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceNo ratings yet
- Up in Smoke: How the Retirement Crisis Shattered the American DreamFrom EverandUp in Smoke: How the Retirement Crisis Shattered the American DreamNo ratings yet
- Q Aworking HoursDocument9 pagesQ Aworking HoursOm PrakashNo ratings yet
- 6 IpeDocument46 pages6 IpeFarhan NawazNo ratings yet
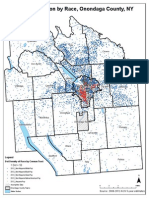
- CNY Segregation MapsDocument13 pagesCNY Segregation MapsTim KnaussNo ratings yet
- Pareto EfficiencyDocument2 pagesPareto EfficiencyGroup_G100% (1)
- Delegated LegislationDocument20 pagesDelegated LegislationAmit Singh100% (5)
- Authorization For Salary ChangeDocument2 pagesAuthorization For Salary ChangeKhan Mohammad Mahmud HasanNo ratings yet
- Circular 13 2019Document2 pagesCircular 13 2019Tejindar SinghNo ratings yet
- Atal Pension Yojana (Apy) - Subscriber Registration FormDocument1 pageAtal Pension Yojana (Apy) - Subscriber Registration FormMk SinghNo ratings yet
- Total Rewards - 3012019Document3 pagesTotal Rewards - 3012019AmanNo ratings yet
- Homework MicroeconomicsDocument4 pagesHomework MicroeconomicsNguyễn Bảo Ngọc100% (1)
- Chapter 1 BASIC ECONOMIC CONCEPTDocument19 pagesChapter 1 BASIC ECONOMIC CONCEPTMuhammad FirdausNo ratings yet
- Ranking Template For Master Teacher 2Document1 pageRanking Template For Master Teacher 2Kimberly Ann Moscare AntoNo ratings yet
- 2131Document2 pages2131Jeffrey JenNo ratings yet
- UNICEF: The State of The World's Children 1988Document98 pagesUNICEF: The State of The World's Children 1988UNICEFNo ratings yet
- The Problem of Youth OffendersDocument3 pagesThe Problem of Youth OffendersAmina JavierNo ratings yet
- 2017 HHS Poverty Guidelines For Affidavit of SupportDocument1 page2017 HHS Poverty Guidelines For Affidavit of SupportLiz MNo ratings yet
- Chapter 23Document22 pagesChapter 23api-261513952No ratings yet
- Concept of Liberty: Its Emergence & EvolutionDocument16 pagesConcept of Liberty: Its Emergence & EvolutionBalaji P Nadar100% (1)
- Definitions of SOE, GLC, GLIC & CLBGDocument2 pagesDefinitions of SOE, GLC, GLIC & CLBGGinger Kalaivani0% (1)
- Monologue by Aaron SorkinDocument2 pagesMonologue by Aaron SorkinsiddharthNo ratings yet
- MS34Document2 pagesMS34Narasimha SastryNo ratings yet
- Distributive Justice AO3Document3 pagesDistributive Justice AO3pogletNo ratings yet
- Oddfellows HistoryDocument10 pagesOddfellows HistoryFuzzy_Wood_Person100% (1)
- Where Does The Money Go? Funding For Indigenous HealthDocument2 pagesWhere Does The Money Go? Funding For Indigenous HealthdiamondphoenixNo ratings yet
- Factor Proportions Theory of International TradeDocument2 pagesFactor Proportions Theory of International TradehymonicaNo ratings yet
- RPW Day 3Document2 pagesRPW Day 3Isah MiguelNo ratings yet
- Becker-A Theory of Competition Among Pressure Groups For Political InfluenceDocument31 pagesBecker-A Theory of Competition Among Pressure Groups For Political InfluenceJaime Luis Zapata GarciaNo ratings yet
- Ex EsmDocument2 pagesEx Esmmurty ch.sNo ratings yet
- Inventory of Bank Accounts As of June 2019Document96 pagesInventory of Bank Accounts As of June 2019Tim PuertosNo ratings yet
- Amartya Sen's View of Economic DevelopmentDocument6 pagesAmartya Sen's View of Economic DevelopmentFaisal AhmedNo ratings yet