You might also like
- CT Physics for Quality and Dose OptimizationDocument75 pagesCT Physics for Quality and Dose OptimizationdanaNo ratings yet
- CT Dose IssuesDocument28 pagesCT Dose IssuessanyengereNo ratings yet
- Radiological Equipment: Assignment Presentation On Several TopicsDocument58 pagesRadiological Equipment: Assignment Presentation On Several TopicsAsteway MesfinNo ratings yet
- CT Radiation Dose and Image Quality: J. Thomas Payne, PHDTDocument10 pagesCT Radiation Dose and Image Quality: J. Thomas Payne, PHDTradiologi rsudNo ratings yet
- Advanced Topics in Biomedical EngineeringDocument35 pagesAdvanced Topics in Biomedical EngineeringAmmer SaifullahNo ratings yet
- TM 10. CT CARDIAC Artikel 2 PCD-CTDocument13 pagesTM 10. CT CARDIAC Artikel 2 PCD-CTrellvandraaaNo ratings yet
- Cardiac Computed Tomography Technology PDFDocument73 pagesCardiac Computed Tomography Technology PDFRamona GhengheaNo ratings yet
- Medical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyDocument13 pagesMedical Physics - 2018 - Ommen - Image Quality of Conventional Images of Dual Layer SPECTRAL CT A Phantom StudyAmril MukminNo ratings yet
- Zoology ProjectDocument9 pagesZoology ProjectPorkodi ShanmugamNo ratings yet
- Strategies For Radiation Dose OptimizationDocument10 pagesStrategies For Radiation Dose OptimizationthutaNo ratings yet
- Engleski Jezik Amar AscericDocument10 pagesEngleski Jezik Amar AscericArminNo ratings yet
- Huda 2010Document7 pagesHuda 2010Roshi_11No ratings yet
- Ctscanfinal2 160709063902Document60 pagesCtscanfinal2 160709063902Abegail IbañezNo ratings yet
- Advanced Imaging TechniquesDocument39 pagesAdvanced Imaging Techniquesjenny girl100% (1)
- CT Scan Vs MRI - Difference Tabular FormDocument6 pagesCT Scan Vs MRI - Difference Tabular FormSana chaudharyNo ratings yet
- How Iodine Uptake Affects Radiation Dose in Contrast-Enhanced CTDocument8 pagesHow Iodine Uptake Affects Radiation Dose in Contrast-Enhanced CTJose Mateo Baron RestrepoNo ratings yet
- CT Radiation Dose and Radiation Reduction Strategies: Focused Issue of This MonthDocument7 pagesCT Radiation Dose and Radiation Reduction Strategies: Focused Issue of This MonthHarley Alejo MNo ratings yet
- Solution Manual COUGHANOWRDocument42 pagesSolution Manual COUGHANOWRKandarp KaushikNo ratings yet
- Comparison ChartDocument4 pagesComparison Chartmuhammed progerNo ratings yet
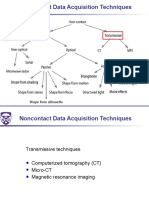
- 08 No Contact Data Asquisition Misc 2019 09 19Document47 pages08 No Contact Data Asquisition Misc 2019 09 19TimNo ratings yet
- TAC PeñascoDocument10 pagesTAC PeñascoJose ManuelNo ratings yet
- Photon Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging ApplicationDocument27 pagesPhoton Counting Spectral CT Versus Conventional CT: Comparative Evaluation For Breast Imaging Applicationcarlos56dbNo ratings yet
- Dual-Source CT and The Effect of Tin Filtration On ImageDocument6 pagesDual-Source CT and The Effect of Tin Filtration On Imagemas bejo01No ratings yet
- CT Activity No.1 - BordonDocument4 pagesCT Activity No.1 - BordonVIDMENTON PHNo ratings yet
- Principles of CT Scan AbdomenDocument101 pagesPrinciples of CT Scan Abdomenrajan kumar100% (16)
- X-Ray Imaging Class - 3Document22 pagesX-Ray Imaging Class - 3HaylishaNo ratings yet
- Tool and EquipmentsDocument10 pagesTool and EquipmentsKhafidzul Fiqih Reviyant TohaNo ratings yet
- Medical Uses of Ionising RadiationDocument42 pagesMedical Uses of Ionising Radiationsyafieq_syaf937438No ratings yet
- Lecture Medical ImagingDocument85 pagesLecture Medical Imagingpiterwisely100% (1)
- Radiation and Nuclear MedicineDocument29 pagesRadiation and Nuclear MedicineGoran MaliNo ratings yet
- X-Ray Computed Tomography of The HeartDocument19 pagesX-Ray Computed Tomography of The Heartbdalcin5512No ratings yet
- New Techniques in RadiotherapyDocument134 pagesNew Techniques in Radiotherapycrusader888100% (1)
- Principles of CT and CT Technology : P CT CTT - Goldman 115Document14 pagesPrinciples of CT and CT Technology : P CT CTT - Goldman 115Madalina ConstantinNo ratings yet
- Basic Physics of MSCT: Radiodiagnostic and RadioteraphyDocument94 pagesBasic Physics of MSCT: Radiodiagnostic and Radioteraphyardi wijanaNo ratings yet
- Acceptance Test and Clinical Commissioning of CT SDocument8 pagesAcceptance Test and Clinical Commissioning of CT SEskadmas BelayNo ratings yet
- Quantification of Cross Vendor Variation in ADC MeDocument6 pagesQuantification of Cross Vendor Variation in ADC MedeaNo ratings yet
- CT Scans: and Their ApplicationDocument44 pagesCT Scans: and Their ApplicationAmi JeebaNo ratings yet
- Radiation Dose and Cancer Risk in RetrospectivelyDocument8 pagesRadiation Dose and Cancer Risk in RetrospectivelyCristiam Guillermo UzuriagaNo ratings yet
- CT SacnDocument6 pagesCT SacnmartinNo ratings yet
- CT Radiation ProtectionDocument8 pagesCT Radiation ProtectionKhush JainNo ratings yet
- Medical Imaging Modalities: X-ray, CT, PET, Ultrasound, MRIDocument47 pagesMedical Imaging Modalities: X-ray, CT, PET, Ultrasound, MRIEduardo BartolomeNo ratings yet
- Exposure Chart Mobile X Ray PDFDocument8 pagesExposure Chart Mobile X Ray PDFlutfiaNo ratings yet
- J. Nucl. Med. Technol. 2007 Goldman 115 28Document15 pagesJ. Nucl. Med. Technol. 2007 Goldman 115 28Ruxandra LúthienNo ratings yet
- PET Scan Costs $3K-$6K, Reveals Biological ProcessesDocument3 pagesPET Scan Costs $3K-$6K, Reveals Biological ProcessesJustine PlazaNo ratings yet
- Computed TomographyDocument2 pagesComputed TomographyemilyNo ratings yet
- Principles of CT and CT TechnologyDocument15 pagesPrinciples of CT and CT TechnologyLida Velasquez SierraNo ratings yet
- Utilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainDocument4 pagesUtilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainJorge RodriguezNo ratings yet
- Computed Tomography or CT Scanning of The Heart (CT Coronary Angiogram) Is A ProcedureDocument4 pagesComputed Tomography or CT Scanning of The Heart (CT Coronary Angiogram) Is A ProcedureYugendra Babu KNo ratings yet
- Positron Emission Tomography - pg1018Document37 pagesPositron Emission Tomography - pg1018HammadNo ratings yet
- Multi-Modal CT Scanning in The Evaluation of Cerebrovascular Disease PatientsDocument18 pagesMulti-Modal CT Scanning in The Evaluation of Cerebrovascular Disease PatientsmicozaaaNo ratings yet
- Gamma CameraDocument26 pagesGamma CameraNishtha TanejaNo ratings yet
- Final OneDocument63 pagesFinal OneAmanda TeacaNo ratings yet
- Zanzonico 2008Document17 pagesZanzonico 2008martuflashNo ratings yet
- What Is Cone Beam Computed Tomography (CBCT) ?Document1 pageWhat Is Cone Beam Computed Tomography (CBCT) ?224edgeb100% (2)
- CT Scan PPT ReportDocument12 pagesCT Scan PPT ReportAljon Zairel LasalaNo ratings yet
- A Dose-Neutral Image Quality Comparison of Different CBCT and CT Systems Using Paranasal Sinus Imaging Protocols and PhantomsDocument8 pagesA Dose-Neutral Image Quality Comparison of Different CBCT and CT Systems Using Paranasal Sinus Imaging Protocols and Phantomsmarito’No ratings yet
- Radiol 2018172656Document20 pagesRadiol 2018172656rnjNo ratings yet
- Biomedical imaging techniques and applicationsDocument63 pagesBiomedical imaging techniques and applicationsYlrebmik ArrabiNo ratings yet
- Letter To DoctorsDocument3 pagesLetter To Doctorsjason9486No ratings yet
- Radiation Dose Compared Too The SourcesDocument2 pagesRadiation Dose Compared Too The Sourcesjason9486No ratings yet
- Letter To DoctorsDocument3 pagesLetter To Doctorsjason9486No ratings yet
- Jama ClassificationDocument8 pagesJama Classificationjason9486No ratings yet
- Jama PredictorDocument3 pagesJama Predictorjason9486No ratings yet
- Non Invasive CT Coronary Artery ImagingDocument43 pagesNon Invasive CT Coronary Artery Imagingjason9486No ratings yet
- Non Invasive CT Coronary Artery ImagingDocument43 pagesNon Invasive CT Coronary Artery Imagingjason9486No ratings yet
- Radiology Imaging in Cochlear Implant Preparation PDFDocument50 pagesRadiology Imaging in Cochlear Implant Preparation PDFrizaNo ratings yet
- JSUMC FPPE Focused Professional Practice EvalDocument9 pagesJSUMC FPPE Focused Professional Practice EvalDwi cahyaniNo ratings yet
- Magical Passes: The Practical Wisdom of The Shamans of Ancient MexicoDocument3 pagesMagical Passes: The Practical Wisdom of The Shamans of Ancient MexicoTyler HiggsNo ratings yet
- Yes This Is A TitleDocument8 pagesYes This Is A TitleIzzHyukNo ratings yet
- Phs Mammographer PresentationDocument10 pagesPhs Mammographer Presentationapi-546893338No ratings yet
- Sree Chitra Tirunal Institute Course CurriculumsDocument55 pagesSree Chitra Tirunal Institute Course Curriculumsfindingnemo667No ratings yet
- Optima CT520Document24 pagesOptima CT520Mario RamosNo ratings yet
- Anthony Filly CVDocument5 pagesAnthony Filly CVapi-289727140No ratings yet
- The AnswerDocument24 pagesThe AnswerrezokaNo ratings yet
- CPG Cap 2010Document12 pagesCPG Cap 2010RenatoCosmeGalvanJuniorNo ratings yet
- Nuclear Medical Technologist Medicine in Chicago IL Resume Marianne VanekDocument1 pageNuclear Medical Technologist Medicine in Chicago IL Resume Marianne VanekMarianneVanekNo ratings yet
- X-Ray Safety ManualDocument34 pagesX-Ray Safety ManualAhmed AssafNo ratings yet
- Engleski Jezik Amar AscericDocument10 pagesEngleski Jezik Amar AscericArminNo ratings yet
- Pemeriksaan Radiologi Trauma ThoraxDocument6 pagesPemeriksaan Radiologi Trauma ThoraxshabrinaNo ratings yet
- Supafly PaperDocument4 pagesSupafly Paperapi-404851310No ratings yet
- Thesis Radiologic TechnologyDocument8 pagesThesis Radiologic Technologytinajordanhuntsville100% (2)
- Adapted Anatomical Image Criteria For PA Chest RadiographyDocument29 pagesAdapted Anatomical Image Criteria For PA Chest RadiographyDR MUHAMMAD NADEEMNo ratings yet
- Jurnal PediatricDocument9 pagesJurnal PediatricDian Angraeni WidiastutiNo ratings yet
- Kuliah Radiologi Emergensi - Maret 2020 - PlainDocument67 pagesKuliah Radiologi Emergensi - Maret 2020 - PlainArief VerditoNo ratings yet
- Frizell A Benton Transition To Itresume 2013Document2 pagesFrizell A Benton Transition To Itresume 2013api-218516728No ratings yet
- Aimcat 2011Document114 pagesAimcat 2011Mansit SumanNo ratings yet
- Radiologic Technology: As A ProfessionDocument30 pagesRadiologic Technology: As A ProfessionKim MngcupaNo ratings yet
- Interventional Pain ManagementDocument637 pagesInterventional Pain Managementatika sgrt0% (1)
- NeuroimagingDocument47 pagesNeuroimagingKertiasihwayan100% (1)
- A Practical Guide To Artificial Intelligence-Based Image Analysis in RadiologyDocument7 pagesA Practical Guide To Artificial Intelligence-Based Image Analysis in RadiologyGeneNo ratings yet
- Methods For Evaluating Common RadiologyDocument13 pagesMethods For Evaluating Common Radiologyapi-434957773No ratings yet
- Mean filter and median filter for lung cancer detection using digital image processingDocument41 pagesMean filter and median filter for lung cancer detection using digital image processingSaidhaNo ratings yet
- Cirse 2016Document352 pagesCirse 2016huwahuNo ratings yet
- Non-Metallic Grid For Radiographs PPT by DR - AliDocument29 pagesNon-Metallic Grid For Radiographs PPT by DR - Alisyed.khaja ali uddinNo ratings yet
- Brosur TrilogyDocument7 pagesBrosur TrilogyHendra SetiawanNo ratings yet