You might also like
- College of Physicians and Surgeons of Alberta QB1803-01472 Certified Record of Proceedings - Illegal sabotage of Alberta Cancer Therapy Programs and abuse (physical violence, harassment, verbal abuse) of frontline healthcare staff by Alberta NDP and their AHS and CPSA Officials, covered-up by CPSADocument908 pagesCollege of Physicians and Surgeons of Alberta QB1803-01472 Certified Record of Proceedings - Illegal sabotage of Alberta Cancer Therapy Programs and abuse (physical violence, harassment, verbal abuse) of frontline healthcare staff by Alberta NDP and their AHS and CPSA Officials, covered-up by CPSAWilliam MakisNo ratings yet
- OSC Letter To President Barack ObamaDocument6 pagesOSC Letter To President Barack ObamaColoradoanNo ratings yet
- VA Office of Inspector General Interim ReportDocument35 pagesVA Office of Inspector General Interim ReportArthur BarieNo ratings yet
- Office of Inspector GeneralDocument14 pagesOffice of Inspector GeneralJimNo ratings yet
- Office of Inspector GeneralDocument16 pagesOffice of Inspector GeneralJimNo ratings yet
- Community Problem ReportDocument8 pagesCommunity Problem Reportapi-302257492No ratings yet
- Misericordia Hospital Medical Center v. National Labor Relations Board, and Committee of Interns and Residents and New York State Nurses Association, Intervenors-Respondents, 623 F.2d 808, 2d Cir. (1980)Document15 pagesMisericordia Hospital Medical Center v. National Labor Relations Board, and Committee of Interns and Residents and New York State Nurses Association, Intervenors-Respondents, 623 F.2d 808, 2d Cir. (1980)Scribd Government DocsNo ratings yet
- Veterans Health AdministrationDocument143 pagesVeterans Health AdministrationLJ's infoDOCKETNo ratings yet
- Pulmonary MedicineDocument11 pagesPulmonary MedicineMorocotoedNo ratings yet
- Healthcare Inspection Environment of Care and Other Quality Concerns Cincinnati VA Medical Center Cincinnati, OhioDocument15 pagesHealthcare Inspection Environment of Care and Other Quality Concerns Cincinnati VA Medical Center Cincinnati, OhioDan MonkNo ratings yet
- Summary Suspension of Dr. Anthony FarinaDocument21 pagesSummary Suspension of Dr. Anthony FarinaNBC 10 WJARNo ratings yet
- 13-33 DI-12-3816 and DI-13-1713 - Letter To The PresidentDocument22 pages13-33 DI-12-3816 and DI-13-1713 - Letter To The PresidentMichael VolpeNo ratings yet
- OIG Wait Time Report SummaryDocument13 pagesOIG Wait Time Report SummaryDonnieNo ratings yet
- Laney Timeline of VA HarassmentDocument23 pagesLaney Timeline of VA HarassmentArt Levine, Mental Health Inc.No ratings yet
- Research Paper Legal-2Document9 pagesResearch Paper Legal-2Jonathan TranNo ratings yet
- Literature Review Final DraftDocument7 pagesLiterature Review Final Draftapi-266214559No ratings yet
- Johnson V Misericordia Community Hospital Case 2Document3 pagesJohnson V Misericordia Community Hospital Case 2api-253363411No ratings yet
- Johnson V Misericordia Community HospitalDocument4 pagesJohnson V Misericordia Community Hospitalapi-271900931No ratings yet
- Office of Inspector GeneralDocument19 pagesOffice of Inspector GeneralJimNo ratings yet
- United States Court of Appeals, Third CircuitDocument8 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- Vaoig 17 03347 293 PDFDocument37 pagesVaoig 17 03347 293 PDFNewsdayNo ratings yet
- Cheryl Clark, M.D. v. South Broward Hospital District, 11th Cir. (2015)Document31 pagesCheryl Clark, M.D. v. South Broward Hospital District, 11th Cir. (2015)Scribd Government DocsNo ratings yet
- VA Healthcare SystemDocument6 pagesVA Healthcare SystemBillyNo ratings yet
- 16-25-DI-14-3650-DI-13-4570 Agency ReportDocument25 pages16-25-DI-14-3650-DI-13-4570 Agency ReportmikekvolpeNo ratings yet
- Factors and Reviews Affecting Patient Satisfaction in District HospitalsDocument9 pagesFactors and Reviews Affecting Patient Satisfaction in District HospitalsCatherine R. FelipeNo ratings yet
- Factors and Reviews Affecting Patient Satisfaction in District HospitalsDocument9 pagesFactors and Reviews Affecting Patient Satisfaction in District HospitalsCatherine R. FelipeNo ratings yet
- Office of Inspector GeneralDocument20 pagesOffice of Inspector GeneralbradrhenNo ratings yet
- Critical Deficiencies at The Washington DC VA Medical CenterDocument158 pagesCritical Deficiencies at The Washington DC VA Medical CenterAllison MaassNo ratings yet
- Bio-Reference Laboratories Whistle-Blower ComplaintDocument11 pagesBio-Reference Laboratories Whistle-Blower ComplaintBRLIwhistleblower100% (1)
- Medical Malpractice 1 Running Head: Medical Malpractice Are Not ReserveDocument9 pagesMedical Malpractice 1 Running Head: Medical Malpractice Are Not Reservejeannebenfante100% (1)
- In The Matter of Peter J. Delenick, M.D. Before The Maryland State Board of Physicians Case Numbers: 2016-07418 Respondent License Number: D80662Document14 pagesIn The Matter of Peter J. Delenick, M.D. Before The Maryland State Board of Physicians Case Numbers: 2016-07418 Respondent License Number: D80662giyasay671No ratings yet
- Whistleblower Lawsuit, KU HospitalDocument17 pagesWhistleblower Lawsuit, KU HospitalIan CummingsNo ratings yet
- Wrong Medication Near-Miss Analysis (NursingDocument10 pagesWrong Medication Near-Miss Analysis (NursingMaina PeterNo ratings yet
- ComplaintDocument7 pagesComplaintMitchRyalsNo ratings yet
- Stuart Hoven DecisionDocument13 pagesStuart Hoven DecisiondmronlineNo ratings yet
- United States District Court For The District of MarylandDocument23 pagesUnited States District Court For The District of MarylandtinareedreporterNo ratings yet
- Report: Undocumented Patient Care at Chillicothe VA Medical CenterDocument19 pagesReport: Undocumented Patient Care at Chillicothe VA Medical CenterThe Columbus DispatchNo ratings yet
- MDH State Rapid Response Investigative Public Report The Waters On MayowoodDocument13 pagesMDH State Rapid Response Investigative Public Report The Waters On MayowoodinforumdocsNo ratings yet
- AnalisisDocument8 pagesAnalisisAnonymous RPcFL6OVW1No ratings yet
- Journal of Emergency Nursing ArticleDocument12 pagesJournal of Emergency Nursing ArticleJimmy MulkernNo ratings yet
- MCO Lawsuit Court of Appeals OpinionDocument12 pagesMCO Lawsuit Court of Appeals OpinionJustin HinkleyNo ratings yet
- Va'S Current Procedures For Background Checks and CredentialingDocument90 pagesVa'S Current Procedures For Background Checks and CredentialingScribd Government DocsNo ratings yet
- 2020 Suicides in Custody Final With DOC ResponseDocument20 pages2020 Suicides in Custody Final With DOC ResponsePG EdiNo ratings yet
- Features of Online Hospital Appointment Systems in Taiwan: A Nationwide SurveyDocument10 pagesFeatures of Online Hospital Appointment Systems in Taiwan: A Nationwide SurveyJayaprada S. HiremathNo ratings yet
- Kerry Heinecke Med Inf 407 - Group Case Study Project Case Study #1Document6 pagesKerry Heinecke Med Inf 407 - Group Case Study Project Case Study #1api-106423440No ratings yet
- Improving Healthcare OrganizationDocument5 pagesImproving Healthcare OrganizationEvans MunyaoNo ratings yet
- Covid-19 - Researcher Blows The Whistle On Data Integrity Issues in Pfizer's Vaccine Trial - The BMJDocument10 pagesCovid-19 - Researcher Blows The Whistle On Data Integrity Issues in Pfizer's Vaccine Trial - The BMJtyakimisNo ratings yet
- Criminal Complaint State of Wisconsin v. Armor Correctional Health Services, Inc.Document11 pagesCriminal Complaint State of Wisconsin v. Armor Correctional Health Services, Inc.CHRISTINA CURRIENo ratings yet
- Decline To SignDocument6 pagesDecline To SignShirley Pigott MDNo ratings yet
- 34 CueDocument6 pages34 Cuejim912No ratings yet
- Textbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationFrom EverandTextbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationNo ratings yet
- How Hockey Can Save Healthcare: A Principle - Based Approach to Reforming the Canadian Healthcare SystemFrom EverandHow Hockey Can Save Healthcare: A Principle - Based Approach to Reforming the Canadian Healthcare SystemNo ratings yet
- Healthcare Applications: A Casebook in Accounting and Financial ManagementFrom EverandHealthcare Applications: A Casebook in Accounting and Financial ManagementNo ratings yet
- Risk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsFrom EverandRisk Management and the Emergency Department: Executive Leadership for Protecting Patients and HospitalsNo ratings yet
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareFrom EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareNo ratings yet
- The History and Transformation of the California Workers’ Compensation System and the Impact of Senate Bill 899 and the Current Law Senate Bill 863From EverandThe History and Transformation of the California Workers’ Compensation System and the Impact of Senate Bill 899 and the Current Law Senate Bill 863No ratings yet
- Guide to the Code of Ethics for Nurses: Interpretation and ApplicationFrom EverandGuide to the Code of Ethics for Nurses: Interpretation and ApplicationNo ratings yet
- Textbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionFrom EverandTextbook of Urgent Care Management: Chapter 41, Measuring and Improving Patient SatisfactionNo ratings yet
- Brent Brennan ContractDocument5 pagesBrent Brennan ContractKOLD News 13No ratings yet
- University of Arizona Public Case DecisionDocument122 pagesUniversity of Arizona Public Case DecisionKOLD News 13No ratings yet
- 1.18.24 Letter To DOJ Re Facial Recognition and Title VIDocument6 pages1.18.24 Letter To DOJ Re Facial Recognition and Title VILindsey BasyeNo ratings yet
- Autopsy Report For Wade WelchDocument8 pagesAutopsy Report For Wade WelchKOLD News 13No ratings yet
- Gov. Hobbs Letter To Lawmakers About CRT BillDocument2 pagesGov. Hobbs Letter To Lawmakers About CRT BillKOLD News 13No ratings yet
- 2022-12-2 Cochise BOS ReferralDocument3 pages2022-12-2 Cochise BOS ReferralKOLD News 13No ratings yet
- Letter To Pima County Board of SupervisorsDocument3 pagesLetter To Pima County Board of SupervisorsKOLD News 13No ratings yet
- IARP News ReleaseDocument13 pagesIARP News ReleaseKOLD News 13No ratings yet
- Grijalva Letter To WH&DHS 5.12.2023Document1 pageGrijalva Letter To WH&DHS 5.12.2023KOLD News 13No ratings yet
- Report Cards For Southern Arizona SchoolsDocument12 pagesReport Cards For Southern Arizona SchoolsKOLD News 13No ratings yet
- Active Shooter Incidents in The Us 2022 042623Document33 pagesActive Shooter Incidents in The Us 2022 042623KOLD News 13No ratings yet
- 2022-12-2 Cochise BOS ReferralDocument3 pages2022-12-2 Cochise BOS ReferralKOLD News 13No ratings yet
- Arizona's Academic Standards Assessment Scores For Pima CountyDocument2 pagesArizona's Academic Standards Assessment Scores For Pima CountyKOLD News 13No ratings yet
- Yuma Morelos Dam Notification Letter ENGLISHDocument2 pagesYuma Morelos Dam Notification Letter ENGLISHKOLD News 13No ratings yet
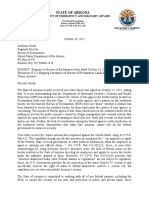
- Response To BOR Oct-18-2022-122 Shipping Containers in YumaDocument2 pagesResponse To BOR Oct-18-2022-122 Shipping Containers in YumaKOLD News 13No ratings yet
- AERC HLC Complaint - October 7 2022Document1 pageAERC HLC Complaint - October 7 2022KOLD News 13No ratings yet
- 2022-11-28 Complaint For Special ActionDocument53 pages2022-11-28 Complaint For Special ActionKOLD News 13No ratings yet
- PCCEA Complaint To HLC - Oct 8 2022Document2 pagesPCCEA Complaint To HLC - Oct 8 2022KOLD News 13100% (1)
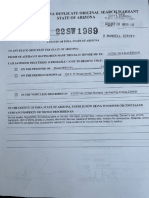
- Search Warrant For Murad Can DervishDocument14 pagesSearch Warrant For Murad Can DervishKOLD News 13No ratings yet
- HLC Final ReportDocument3 pagesHLC Final ReportKOLD News 13No ratings yet
- Dervish Interim Complaint (Redacted)Document2 pagesDervish Interim Complaint (Redacted)KOLD News 13No ratings yet
- 2022 08 30 State V City of Tucson ComplaintDocument15 pages2022 08 30 State V City of Tucson ComplaintKOLD News 13No ratings yet
- Waller ComplaintDocument29 pagesWaller ComplaintKOLD News 13No ratings yet
- 2022 Maui Invitational BracketDocument1 page2022 Maui Invitational BracketKOLD News 13No ratings yet
- Pima County Vote Centers For Aug. 2, 2022 ElectionDocument2 pagesPima County Vote Centers For Aug. 2, 2022 ElectionKOLD News 13No ratings yet
- PIO - San - Rafael 5 - 9Document1 pagePIO - San - Rafael 5 - 9KOLD News 13No ratings yet
- TVUSD Statement - Gary Lewis, TVHS Athletic Director - April 1, 2022Document1 pageTVUSD Statement - Gary Lewis, TVHS Athletic Director - April 1, 2022KOLD News 13No ratings yet
- 2022-07-22 Source of Income Ordinance (Redline)Document3 pages2022-07-22 Source of Income Ordinance (Redline)KOLD News 13No ratings yet
- TVUSD Statement - Graffiti Incident, April 1, 2022Document2 pagesTVUSD Statement - Graffiti Incident, April 1, 2022KOLD News 13No ratings yet
- Ducey EmailDocument2 pagesDucey EmailKOLD News 13No ratings yet
- Role of Nurses in Health Care SystemDocument1 pageRole of Nurses in Health Care Systemcadolly carnoiseNo ratings yet
- Newborn AssessmentDocument9 pagesNewborn Assessmentapi-237668254No ratings yet
- Duties and Responsibilities of An RN: Lpns CnasDocument4 pagesDuties and Responsibilities of An RN: Lpns CnasSPTDNo ratings yet
- Social Worker or MSW or LCSW or LCADCDocument2 pagesSocial Worker or MSW or LCSW or LCADCapi-77399086No ratings yet
- Helen K. Sneller: Program, 1996Document2 pagesHelen K. Sneller: Program, 1996Siddharth NelsonNo ratings yet
- Danger Signs in Pregnancy Teaching PlanDocument6 pagesDanger Signs in Pregnancy Teaching PlanEn George88% (8)
- No Balance Billing PolicyDocument6 pagesNo Balance Billing PolicyRhyne Amante YpulongNo ratings yet
- Management of Sacral Dimples Detected On Routine Newborn Examination: A Case Series and ReviewDocument3 pagesManagement of Sacral Dimples Detected On Routine Newborn Examination: A Case Series and ReviewDesta FransiscaNo ratings yet
- CIC Approved Panel - of Medical Service Providers PDFDocument11 pagesCIC Approved Panel - of Medical Service Providers PDFjohnson mwauraNo ratings yet
- Founder Fellows of Tamilnadu Academy of SciencesDocument5 pagesFounder Fellows of Tamilnadu Academy of SciencesPonnusamy RamalingamNo ratings yet
- Knights HospitallerDocument14 pagesKnights HospitallerAlison_VicarNo ratings yet
- Tracy Hawthorne Wayne State Resume 2 3 15 16Document3 pagesTracy Hawthorne Wayne State Resume 2 3 15 16api-318418964No ratings yet
- Dr. Rubi Li Vs Spouses Reynaldo and Lina Soliman GR NO. 165279 - JUNE 7, 2011 Villarama, JR.,JDocument10 pagesDr. Rubi Li Vs Spouses Reynaldo and Lina Soliman GR NO. 165279 - JUNE 7, 2011 Villarama, JR.,JthelawbeanNo ratings yet
- 2016 Annual Report PDFDocument70 pages2016 Annual Report PDFkipumNo ratings yet
- Provisional Restoration Options in Implant DentistryDocument8 pagesProvisional Restoration Options in Implant Dentistrydevendra chhonkarNo ratings yet
- 01 2012Document17 pages01 2012Yuie Clemente Sta CruzNo ratings yet
- Nursing ApplicationDocument1 pageNursing ApplicationGuru JiNo ratings yet
- Healthcare HRM 2e PPT CH 01Document15 pagesHealthcare HRM 2e PPT CH 01Gumz100% (2)
- Scheduling Patients' Appointments: Allocation of Healthcare Service Using Simulation OptimizationDocument23 pagesScheduling Patients' Appointments: Allocation of Healthcare Service Using Simulation OptimizationAnonymous 3DjVNbNo ratings yet
- MS3 Student Survival GuideDocument18 pagesMS3 Student Survival GuideNoah ThomasNo ratings yet
- English NIOS Class12 April 2015Document15 pagesEnglish NIOS Class12 April 2015chhotuNo ratings yet
- Not-Installed Medical Equipment List of All Hospital in Jimma Zone Full InfoDocument58 pagesNot-Installed Medical Equipment List of All Hospital in Jimma Zone Full Infomisgana etichaNo ratings yet
- Flood Preparedness Guidelines for Mumbai Ward DDocument10 pagesFlood Preparedness Guidelines for Mumbai Ward DAkshayRautNo ratings yet
- Hospital/Clinic Management System: Table of ContentsDocument4 pagesHospital/Clinic Management System: Table of ContentsmanofdecadeNo ratings yet
- 1883 - 17 E GamesDocument22 pages1883 - 17 E GamesMohamed Rikarz Ahamed Rikarz100% (1)
- Diagnostic Labs List PHDocument65 pagesDiagnostic Labs List PHgreghalol2017No ratings yet
- Eating Attitudes Test (EAT-40) J-swinbourne-ThesisDocument442 pagesEating Attitudes Test (EAT-40) J-swinbourne-ThesisMilosNo ratings yet
- CDC UP Project Charter TemplateDocument7 pagesCDC UP Project Charter TemplateMasters PMNo ratings yet
- Sentinel Event PaperDocument12 pagesSentinel Event Paperapi-285998412No ratings yet
- Introduction To Jung - Frieda FordhamDocument89 pagesIntroduction To Jung - Frieda Fordhamsolonielle123100% (1)