You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Mac Wellman - The Lesser MagooDocument86 pagesMac Wellman - The Lesser MagooOmar WilleyNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Human Resource Management (Assignment)Document8 pagesHuman Resource Management (Assignment)Engr Muhammad EhsanNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Eight Urban Ministry Strategies.150195235Document9 pagesEight Urban Ministry Strategies.150195235m28181920100% (2)
- Chapter Mentoring HandbookDocument15 pagesChapter Mentoring HandbookSwaa Upchaar100% (3)
- Operation Mind Control - 1Document157 pagesOperation Mind Control - 1marc100% (1)
- Disney's Beauty and the Beast Challenges Gender StereotypesDocument9 pagesDisney's Beauty and the Beast Challenges Gender StereotypesmsyakirkNo ratings yet
- Great Brain TeasersDocument10 pagesGreat Brain TeasersMindy LooNo ratings yet
- Reviewer in Public CorpDocument26 pagesReviewer in Public CorpJerome Delos ReyesNo ratings yet
- Demos-Moving Images of GlobalizationDocument24 pagesDemos-Moving Images of GlobalizationEmanuel Almborg100% (1)
- Deed of Sale (Guns) - SampleDocument3 pagesDeed of Sale (Guns) - Samplealaricelyang0% (1)
- FY 18-19 Budget School Aid RunsDocument15 pagesFY 18-19 Budget School Aid RunsMatthew HamiltonNo ratings yet
- SNY0118 Crosstabs011618Document7 pagesSNY0118 Crosstabs011618Nick ReismanNo ratings yet
- 2018-19 Executive Budget Briefing BookDocument161 pages2018-19 Executive Budget Briefing BookMatthew Hamilton100% (1)
- IDC Leader Jeff Klein Legal Memo Re: Sexual Harassment Allegation.Document3 pagesIDC Leader Jeff Klein Legal Memo Re: Sexual Harassment Allegation.liz_benjamin6490No ratings yet
- SNY0118 Crosstabs011518Document3 pagesSNY0118 Crosstabs011518Matthew HamiltonNo ratings yet
- Joint Budget Schedule 2018 Release FINALDocument1 pageJoint Budget Schedule 2018 Release FINALMatthew HamiltonNo ratings yet
- New York State Plastic Bag Task Force ReportDocument88 pagesNew York State Plastic Bag Task Force ReportMatthew Hamilton100% (1)
- State of The State BingoDocument5 pagesState of The State BingoMatthew Hamilton100% (1)
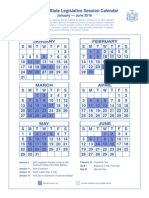
- 2016 Legislative Session CalendarDocument1 page2016 Legislative Session CalendarMatthew HamiltonNo ratings yet
- DiNapoli Debt Impact Study 2017Document30 pagesDiNapoli Debt Impact Study 2017Matthew HamiltonNo ratings yet
- 2018 State of The State BookDocument374 pages2018 State of The State BookMatthew HamiltonNo ratings yet
- 6-22-17 Heastie Letter To Ethics Committee Re: McLaughlin InvestigationDocument1 page6-22-17 Heastie Letter To Ethics Committee Re: McLaughlin InvestigationMatthew HamiltonNo ratings yet
- 6-21-17 Ethics Committee Letter To Heastie Re: McLaughlin InvestigationDocument3 pages6-21-17 Ethics Committee Letter To Heastie Re: McLaughlin InvestigationMatthew HamiltonNo ratings yet
- Approval #64-66 of 2017Document3 pagesApproval #64-66 of 2017Matthew HamiltonNo ratings yet
- 11-27-17 LetterDocument5 pages11-27-17 LetterNick ReismanNo ratings yet
- Andrew Cuomo Letter To Jeff Bezos Re HQ2Document2 pagesAndrew Cuomo Letter To Jeff Bezos Re HQ2Matthew HamiltonNo ratings yet
- 11-29-17 Heastie Letter To McLaughlin Re: McLaughlin InvestigationDocument2 pages11-29-17 Heastie Letter To McLaughlin Re: McLaughlin InvestigationMatthew HamiltonNo ratings yet
- SNY1017 CrosstabsDocument6 pagesSNY1017 CrosstabsNick ReismanNo ratings yet
- USA v. Skelos Appellate DecisionDocument12 pagesUSA v. Skelos Appellate DecisionMatthew HamiltonNo ratings yet
- Comptroller's Fiscal Update: State Fiscal Year 2017-18 Receipts and Disbursements Through The Mid-YearDocument10 pagesComptroller's Fiscal Update: State Fiscal Year 2017-18 Receipts and Disbursements Through The Mid-YearMatthew HamiltonNo ratings yet
- DiNapoli Wall Street Profits Report 2017Document8 pagesDiNapoli Wall Street Profits Report 2017Matthew HamiltonNo ratings yet
- NYS DFS Credit Reporting Agency RegulationsDocument6 pagesNYS DFS Credit Reporting Agency RegulationsMatthew HamiltonNo ratings yet
- DiNapoli Federal Budget ReportDocument36 pagesDiNapoli Federal Budget ReportMatthew HamiltonNo ratings yet
- OSC Municipal Water Systems ReportDocument14 pagesOSC Municipal Water Systems ReportMatthew HamiltonNo ratings yet
- USA V Pigeon 100617Document29 pagesUSA V Pigeon 100617Matthew HamiltonNo ratings yet
- Siena College October 2017 PollDocument8 pagesSiena College October 2017 PollMatthew HamiltonNo ratings yet
- Rockefeller Instittue 106 Ideas For A Constitutional ConventionDocument17 pagesRockefeller Instittue 106 Ideas For A Constitutional ConventionMatthew HamiltonNo ratings yet
- Gov. Andrew Immigration Status Executive OrderDocument2 pagesGov. Andrew Immigration Status Executive OrderMatthew HamiltonNo ratings yet
- Faso Scaffold Law BillDocument4 pagesFaso Scaffold Law BillMatthew HamiltonNo ratings yet
- Gov. Andrew Cuomo Law Approval Message #6 - 2017Document1 pageGov. Andrew Cuomo Law Approval Message #6 - 2017Matthew HamiltonNo ratings yet
- Essay The Old Man and The SeaDocument2 pagesEssay The Old Man and The SeaAlina OsorioNo ratings yet
- 169137-2014-Heirs of Sarili v. LagrosaDocument10 pages169137-2014-Heirs of Sarili v. Lagrosajuju_batugalNo ratings yet
- 9.1. People vs. PangilinanDocument36 pages9.1. People vs. PangilinanPatricia SanchezNo ratings yet
- Bacc 401Document10 pagesBacc 401MyMy MargalloNo ratings yet
- Cinema/ldeology/Criticism: Jean-Luc Comolli and Paul NarboniDocument12 pagesCinema/ldeology/Criticism: Jean-Luc Comolli and Paul NarboniLlamil Mena BritoNo ratings yet
- Proclamation of SaleDocument13 pagesProclamation of Salechek86351No ratings yet
- 哈佛大学开放课程 幸福课 (积极心理学) 视频英文字幕下载 (1-12集) (网易公开课提供)Document469 pages哈佛大学开放课程 幸福课 (积极心理学) 视频英文字幕下载 (1-12集) (网易公开课提供)China FcmNo ratings yet
- How Can Whistle-Blowing Prevent Organisational Wrongdoings?: Governance & EthicsDocument19 pagesHow Can Whistle-Blowing Prevent Organisational Wrongdoings?: Governance & EthicsMohamed LisaamNo ratings yet
- Assignment No 1 Philanthropic Dimension of Social ResponsibilityDocument15 pagesAssignment No 1 Philanthropic Dimension of Social ResponsibilitySarim ZiaNo ratings yet
- Part 1 Unit 2 Answer KeyDocument36 pagesPart 1 Unit 2 Answer KeyhossamadelNo ratings yet
- Script For The Role PlayDocument4 pagesScript For The Role Playjoris sulimaNo ratings yet
- Othello EssayDocument4 pagesOthello Essayalexandermarucci17No ratings yet
- Affidavit of WitnessDocument1 pageAffidavit of WitnessCindy-chan DelfinNo ratings yet
- Health Planning AssignmentDocument7 pagesHealth Planning AssignmentShailjaVajpaiNo ratings yet
- Personnel Management Part-IIDocument184 pagesPersonnel Management Part-IIajit704687No ratings yet
- Action Speaks Louder Than WordDocument3 pagesAction Speaks Louder Than Wordnabin bkNo ratings yet
- Vishvantara JatakaDocument8 pagesVishvantara JatakaMilan ShakyaNo ratings yet
- Karapat Dapat by CANVASDocument64 pagesKarapat Dapat by CANVASToki CruzNo ratings yet
- Memorandum of Law RE Shylock CaseDocument13 pagesMemorandum of Law RE Shylock CaseKei Takishima ShengNo ratings yet
- Review Material For Teaching ProfessionDocument16 pagesReview Material For Teaching ProfessionSandy Medyo GwapzNo ratings yet