You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
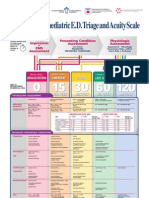
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Forensic Medicine Multiple Choice Question BankDocument20 pagesForensic Medicine Multiple Choice Question BankGIST (Gujarat Institute of Science & Technology)54% (13)
- The Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisDocument10 pagesThe Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisArdi_xNo ratings yet
- X-Ray Toraks Oblik PDFDocument4 pagesX-Ray Toraks Oblik PDFArdi_xNo ratings yet
- Fraktur Tinggi Ramus MandibulaDocument9 pagesFraktur Tinggi Ramus MandibulaArdi_xNo ratings yet
- TB Who 2017Document80 pagesTB Who 2017Yaumul RobbiNo ratings yet
- X RayDocument4 pagesX RayArdi_xNo ratings yet
- TB/HIV Guideline TreatmentDocument6 pagesTB/HIV Guideline TreatmentArdi_xNo ratings yet
- Fraktur Pan FasialDocument5 pagesFraktur Pan FasialArdi_xNo ratings yet
- HIVDocument59 pagesHIVAbdee Negara 'Putra Sahadewa'No ratings yet
- Atrial Septal Defect (ASD) : What Is It?Document3 pagesAtrial Septal Defect (ASD) : What Is It?Gilbert Solomon TantonoNo ratings yet
- Laporan A23Document108 pagesLaporan A23Ardi_xNo ratings yet
- Escala GarfDocument1 pageEscala GarfAna Claudia PoiteNo ratings yet
- Traction (Orthopedics)Document2 pagesTraction (Orthopedics)Sunil PatelNo ratings yet
- Part A: Haley V London Electricity BoardDocument7 pagesPart A: Haley V London Electricity BoardCollins Kipkemoi SangNo ratings yet
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Document10 pagesAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959No ratings yet
- Retrograde Urethrography Examination in Penile Fracture: Case ReportDocument3 pagesRetrograde Urethrography Examination in Penile Fracture: Case Reportsofia ayu lestariNo ratings yet
- Vector D ModelsDocument20 pagesVector D ModelsJose BurritoNo ratings yet
- Common Vocabulary Words for Grades 4-6Document4 pagesCommon Vocabulary Words for Grades 4-6meddana19No ratings yet
- Ergo 4 WeldersDocument32 pagesErgo 4 WeldersjoessterNo ratings yet
- Smith Anna Nicole ReportDocument8 pagesSmith Anna Nicole Reportapi-313225482100% (2)
- Hydraulic Fracture Mechanics: Peter Valk6 Michael EconomidesDocument6 pagesHydraulic Fracture Mechanics: Peter Valk6 Michael EconomidesAdib Wahyu HidayatNo ratings yet
- mn87h JeddahDocument16 pagesmn87h JeddahAlghamdi AlaboudNo ratings yet
- Irrigador InterplakDocument2 pagesIrrigador InterplakCatalina FajardoNo ratings yet
- Calisthenics Training Programs PDFDocument172 pagesCalisthenics Training Programs PDFKhalid SalimNo ratings yet
- Risk AssessmentDocument9 pagesRisk AssessmentTamil SelvanNo ratings yet
- Dhp481z ManualDocument76 pagesDhp481z ManualmmesariciNo ratings yet
- Cluster 3 Pre Board 2022Document19 pagesCluster 3 Pre Board 2022Princess Joy CamposNo ratings yet
- Seizure DisorderDocument36 pagesSeizure DisorderAsniah Hadjiadatu Abdullah100% (1)
- Heroes of HastingtonDocument130 pagesHeroes of HastingtonCostin VidrighinNo ratings yet
- Special Arthrology of The ForelimbDocument37 pagesSpecial Arthrology of The ForelimbTheBoss 20No ratings yet
- Anatomical PositionsDocument39 pagesAnatomical PositionsWaqar AhmedNo ratings yet
- Varicose Vein Care and ExercisesDocument8 pagesVaricose Vein Care and ExercisesAtu KaushalNo ratings yet
- HSE Flyer On Falling Objects April 2018Document4 pagesHSE Flyer On Falling Objects April 2018Perwez21No ratings yet
- Thorax Anatomy..Document21 pagesThorax Anatomy..Dungani AllanNo ratings yet
- ZM-MFC1 Combo: To Ensure Safe and Easy Installation, Please Read The Following PrecautionsDocument7 pagesZM-MFC1 Combo: To Ensure Safe and Easy Installation, Please Read The Following PrecautionsnegatronnNo ratings yet
- Manual Nevera LGDocument28 pagesManual Nevera LGJoher MarquezNo ratings yet
- Mat111 PTDocument7 pagesMat111 PTracyfiloteo11100% (1)
- EELPWAEN0413 Electrical Safety Handbook 20131Document72 pagesEELPWAEN0413 Electrical Safety Handbook 20131abdul samadNo ratings yet
- DKC Spoilers 2875-3217 PDFDocument45 pagesDKC Spoilers 2875-3217 PDFdysryNo ratings yet
- Westside Pro Wrestling - Issue 15 - November 2010Document22 pagesWestside Pro Wrestling - Issue 15 - November 2010api-195949616No ratings yet