You might also like
- Nursing Diagnosis Disturbed Sleep PatternDocument8 pagesNursing Diagnosis Disturbed Sleep Patternmaimai324263100% (2)
- Ugib Case StudyDocument33 pagesUgib Case StudyRosemarie Cunanan Grifoni100% (1)
- COPD ExacerbationDocument12 pagesCOPD ExacerbationJeffrey ShermanNo ratings yet
- Cases For Post Prelims Conference 2009-2010Document7 pagesCases For Post Prelims Conference 2009-2010chocoholic potchi100% (1)
- UN Doctors Directory 2015Document18 pagesUN Doctors Directory 2015Kush GuptaNo ratings yet
- Managing IBD: A Case Study on Diagnosis and TreatmentDocument4 pagesManaging IBD: A Case Study on Diagnosis and TreatmentBejan CorinaNo ratings yet
- Hematochezia Case Report on Crohn's Disease in Young MaleDocument3 pagesHematochezia Case Report on Crohn's Disease in Young Maleseptian_tjayaNo ratings yet
- LepsDocument4 pagesLepslynharee100% (1)
- Penyakit Crohn: Laporan Kasus: Paul V. Siwy, Fandy GosalDocument10 pagesPenyakit Crohn: Laporan Kasus: Paul V. Siwy, Fandy GosalyheyenNo ratings yet
- Typhoid Fever: David T Wheeler, MDDocument14 pagesTyphoid Fever: David T Wheeler, MDChandra KushartantoNo ratings yet
- MainDocument3 pagesMainMila KarmilaNo ratings yet
- Life-Threatening Lower Gastrointestinal Hemorrhage in Pediatric Crohn's DiseaseDocument8 pagesLife-Threatening Lower Gastrointestinal Hemorrhage in Pediatric Crohn's DiseasePeregrine Albertus Ricco AzaliNo ratings yet
- Crohn's Disease and TPNDocument13 pagesCrohn's Disease and TPNAira Vida TesoroNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- Stomach Diseases GuideDocument6 pagesStomach Diseases GuideJames FlanneryNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Case Report: Tuberculosis Liver Abscess in Alcoholism Male PatientDocument4 pagesCase Report: Tuberculosis Liver Abscess in Alcoholism Male PatientWidya Prawirani SiahaanNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (1)
- Pancytopenia Secondary To Bacterial SepsisDocument16 pagesPancytopenia Secondary To Bacterial Sepsisiamralph89No ratings yet
- Pediatric Systemic Lupus Erythematosus Associated With AutoimmuneDocument9 pagesPediatric Systemic Lupus Erythematosus Associated With AutoimmunegistaluvikaNo ratings yet
- Hiding in The Water: Clinical Problem-SolvingDocument6 pagesHiding in The Water: Clinical Problem-SolvingtabareeNo ratings yet
- Hematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewDocument6 pagesHematemesis Melena Due To Helicobacter Pylori Infection in Duodenal Ulcer: A Case Report and Literature ReviewodiNo ratings yet
- Keracunan SianidaDocument8 pagesKeracunan Sianidaclarestatio8No ratings yet
- 54 Shivraj EtalDocument3 pages54 Shivraj EtaleditorijmrhsNo ratings yet
- Case 013: Fever in A Cirrhotic PatientDocument5 pagesCase 013: Fever in A Cirrhotic PatientFitri 1997No ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Development of type I gastric carcinoid in chronic atrophic gastritis patientsDocument9 pagesDevelopment of type I gastric carcinoid in chronic atrophic gastritis patientsAbristaSeptikasariNo ratings yet
- 2013 URINARY TRACT SUMMER REVIEWDocument12 pages2013 URINARY TRACT SUMMER REVIEWJessica MooreNo ratings yet
- 4th Year Write Up 2 - Int. MedDocument11 pages4th Year Write Up 2 - Int. MedLoges TobyNo ratings yet
- Acute Jejunoileal Obstruction Due To A Pseudopolyp in A Child With Undiagnosed Crohn S DiseaseDocument4 pagesAcute Jejunoileal Obstruction Due To A Pseudopolyp in A Child With Undiagnosed Crohn S Diseasebingl_073No ratings yet
- 2019 Article 1205Document6 pages2019 Article 1205zahra h f aNo ratings yet
- Ajol File Journals - 76 - Articles - 114038 - Submission - Proof - 114038 901 318286 1 10 20150309Document2 pagesAjol File Journals - 76 - Articles - 114038 - Submission - Proof - 114038 901 318286 1 10 20150309alysNo ratings yet
- A 31-Year-Old Man With Chronic Cough and HemoptysisDocument6 pagesA 31-Year-Old Man With Chronic Cough and HemoptysiscocomilkNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportAbdullah KhanNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportWyn AgustinNo ratings yet
- Me219 - Haemato CaDocument21 pagesMe219 - Haemato CaAbby LiewNo ratings yet
- Tuberculosis and Chronic Renal FailureDocument38 pagesTuberculosis and Chronic Renal FailureGopal ChawlaNo ratings yet
- 45-Year-Old Man With Shortness of Breath, Cough, and Fever DiagnosisDocument7 pages45-Year-Old Man With Shortness of Breath, Cough, and Fever DiagnosisFluffyyy BabyyyNo ratings yet
- Acalculous Cholecystitis Prevalence On Abdominal Ultrasonography Examination of HIV/HCV Co-Infection Patients in Cipto Mangunkusumo HospitalDocument3 pagesAcalculous Cholecystitis Prevalence On Abdominal Ultrasonography Examination of HIV/HCV Co-Infection Patients in Cipto Mangunkusumo HospitalDiga AlbrianNo ratings yet
- Clin Infect Dis. 2002 Podnos 62 8Document7 pagesClin Infect Dis. 2002 Podnos 62 8nurhasmaryaniNo ratings yet
- Silvajunior 2016Document3 pagesSilvajunior 2016AmatystNo ratings yet
- Literature Review of Chronic Liver DiseaseDocument6 pagesLiterature Review of Chronic Liver Diseaseafmzodjhpxembt100% (1)
- 1471 230X 12 174 PDFDocument5 pages1471 230X 12 174 PDFAila HinlogNo ratings yet
- Crim Em2013-948071Document2 pagesCrim Em2013-948071m.fahimsharifiNo ratings yet
- Background: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSDocument6 pagesBackground: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSSav GaNo ratings yet
- Tuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghDocument3 pagesTuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghAnastasia Lilian SuryajayaNo ratings yet
- Indeterminate ColitisDocument26 pagesIndeterminate ColitisMarlisa YanuartiNo ratings yet
- Case Report: Reynolds SyndromeDocument2 pagesCase Report: Reynolds SyndromePeertechz Publications Inc.No ratings yet
- 0630 - Saturday - SEEK - GrossmanDocument101 pages0630 - Saturday - SEEK - Grossmantechang1No ratings yet
- BMC Dermatology: Schönlein-Henoch Purpura During Pregnancy With Successful Outcome For Mother and NewbornDocument5 pagesBMC Dermatology: Schönlein-Henoch Purpura During Pregnancy With Successful Outcome For Mother and NewbornteguhNo ratings yet
- Case Report Hepato FinalDocument29 pagesCase Report Hepato FinalBangkit PutrawanNo ratings yet
- NewpudpaperDocument15 pagesNewpudpaperapi-2868560640% (1)
- Tuberculous Pleural Effusion Case Study and Literature ReviewDocument3 pagesTuberculous Pleural Effusion Case Study and Literature ReviewtiaanastaNo ratings yet
- The Primary Patient Assessment Form Date Patient Nationality Chief Complaint HPIDocument6 pagesThe Primary Patient Assessment Form Date Patient Nationality Chief Complaint HPIViviaNo ratings yet
- Caso Clinico - AdenocarcinomaDocument1 pageCaso Clinico - AdenocarcinomaXana SoaresNo ratings yet
- Approach For Diagnostic and Treatment of Chronic Diarrhea Caused by Hookworm InfectionDocument7 pagesApproach For Diagnostic and Treatment of Chronic Diarrhea Caused by Hookworm InfectionRianda AkmalNo ratings yet
- Grand Round Presentation on Intestinal TuberculosisDocument40 pagesGrand Round Presentation on Intestinal TuberculosisneptorNo ratings yet
- Case Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasDocument7 pagesCase Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasMudassar SattarNo ratings yet
- Non-Traumatic Rupture of Spleen Can Splenectomy BeDocument3 pagesNon-Traumatic Rupture of Spleen Can Splenectomy Beysh_girlNo ratings yet
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- Price List Artemis Hospital (In Inr) : CardiologyDocument5 pagesPrice List Artemis Hospital (In Inr) : CardiologyKush GuptaNo ratings yet
- CGHS RatesDocument41 pagesCGHS RatesNagesh RaoNo ratings yet
- Laying Marble AreaDocument2 pagesLaying Marble AreaKush GuptaNo ratings yet
- Laying Marble AreaDocument2 pagesLaying Marble AreaKush GuptaNo ratings yet
- Good Health Plays A Major Role in Achieving The Goals.: Test Regularly. Stay Healthy. Keep SucceedingDocument1 pageGood Health Plays A Major Role in Achieving The Goals.: Test Regularly. Stay Healthy. Keep SucceedingKush GuptaNo ratings yet
- Russian EmbassyDocument14 pagesRussian EmbassyKush GuptaNo ratings yet
- Delhi Uni PDFDocument1 pageDelhi Uni PDFKush GuptaNo ratings yet
- Acrylic BookDocument122 pagesAcrylic BookSonia CireaşăNo ratings yet
- Delhi Uni1Document1 pageDelhi Uni1Kush GuptaNo ratings yet
- Wipro BpoDocument10 pagesWipro BpoKush GuptaNo ratings yet
- AIO-publication-40-eng-Final List PDFDocument14 pagesAIO-publication-40-eng-Final List PDFKush GuptaNo ratings yet
- Tor-Sow For Lab For Cnns Draft Dated 9 OctDocument13 pagesTor-Sow For Lab For Cnns Draft Dated 9 OctKush GuptaNo ratings yet
- Ilae IbrocourseprogramfinalDocument5 pagesIlae IbrocourseprogramfinalKush GuptaNo ratings yet
- Dr Lal Pathlabs Invoice #C000662672Document3 pagesDr Lal Pathlabs Invoice #C000662672Kush GuptaNo ratings yet
- Delhi Pathology PanelsDocument1 pageDelhi Pathology PanelsKush GuptaNo ratings yet
- Detail of CFOsDocument4 pagesDetail of CFOsKush Gupta0% (2)
- Delhi UniDocument1 pageDelhi UniKush GuptaNo ratings yet
- Call ReportDocument15 pagesCall ReportKush GuptaNo ratings yet
- Detail of CFOsDocument4 pagesDetail of CFOsKush Gupta0% (2)
- D7C-C2 (Draft CAR Cabin Crew Medical)Document6 pagesD7C-C2 (Draft CAR Cabin Crew Medical)Kush GuptaNo ratings yet
- CGHS Treatment Procedure/Investigation List (New ListDocument3 pagesCGHS Treatment Procedure/Investigation List (New ListKush GuptaNo ratings yet
- Action Plan Corporate - JuneDocument1 pageAction Plan Corporate - JuneKush GuptaNo ratings yet
- Companies Contact Details Amp HR Name 1Document53 pagesCompanies Contact Details Amp HR Name 1srinathssmNo ratings yet
- Action Plan Corporate - JuneDocument1 pageAction Plan Corporate - JuneKush GuptaNo ratings yet
- LocationsDocument1 pageLocationsKush GuptaNo ratings yet
- IPM - Fresh ListDocument15 pagesIPM - Fresh ListKush GuptaNo ratings yet
- DetailDocument2 pagesDetailKush GuptaNo ratings yet
- The Marfan SyndromeDocument6 pagesThe Marfan SyndromeKush GuptaNo ratings yet
- Schonert-Reichl-Educating The Heart As Well As The MindDocument7 pagesSchonert-Reichl-Educating The Heart As Well As The MindnewoldnoneNo ratings yet
- Makna MsiaDocument19 pagesMakna Msiadivaglrboy9023No ratings yet
- Skills - Care of The Pregnant Patient ComputationsDocument5 pagesSkills - Care of The Pregnant Patient ComputationsMichelle HutamaresNo ratings yet
- Agriculture, biotech, bioethics challenges of globalized food systemsDocument28 pagesAgriculture, biotech, bioethics challenges of globalized food systemsperoooNo ratings yet
- Back From The Bluez - 09 - Self ManagementDocument5 pagesBack From The Bluez - 09 - Self ManagementMelanie DovaleNo ratings yet
- 1a - Hernandez - Research PaperDocument28 pages1a - Hernandez - Research PaperEdgar TorresNo ratings yet
- Tanzania STG 052013-Copy 1544379670122Document220 pagesTanzania STG 052013-Copy 1544379670122Waqar WikiNo ratings yet
- Being Single Vs Being MarriedDocument34 pagesBeing Single Vs Being MarriedPeter MissoleNo ratings yet
- Factors Affecting Adherence to Intranasal CorticosteroidsDocument20 pagesFactors Affecting Adherence to Intranasal CorticosteroidsKathrinna Feliz AlertaNo ratings yet
- RCH DEM Head Injury GuidelinesDocument4 pagesRCH DEM Head Injury GuidelinesJerry LeeNo ratings yet
- Principles of Case Planning in Social Work PracticeDocument4 pagesPrinciples of Case Planning in Social Work PracticeJane GilgunNo ratings yet
- Senior High School: Rizal St. Guimbal, IloiloDocument73 pagesSenior High School: Rizal St. Guimbal, IloiloLizbeth Mari MoqueraNo ratings yet
- MIT Medical Department Pediatrics History Form: AppointmentDocument4 pagesMIT Medical Department Pediatrics History Form: Appointmentmaddythedoc100% (1)
- CBT Flashcard Therapy for Schizophrenia PatientsDocument9 pagesCBT Flashcard Therapy for Schizophrenia PatientsMuhammadAjiWicaksonoNo ratings yet
- Lesson 3: Health Information System How Do Health Information Systems Look Like and What Architectures Are Appropriate?Document13 pagesLesson 3: Health Information System How Do Health Information Systems Look Like and What Architectures Are Appropriate?ajengwedaNo ratings yet
- Common Cause or Etiology of Pott's DiseaseDocument5 pagesCommon Cause or Etiology of Pott's DiseaseStan Aves GarciaNo ratings yet
- Assessment of Functional Pain Score by Comparing To Traditional Pain ScoresDocument7 pagesAssessment of Functional Pain Score by Comparing To Traditional Pain ScoresKepompong KupukupuNo ratings yet
- Framework Nurafni SuidDocument2 pagesFramework Nurafni SuidapninoyNo ratings yet
- Cancer Help & Research Trust: Donation AppealDocument1 pageCancer Help & Research Trust: Donation AppealshahrukhsrsNo ratings yet
- Nursing Care Plan: Chronic Pain and COPDDocument11 pagesNursing Care Plan: Chronic Pain and COPDneuronurse100% (1)
- Life Esidimeni Fact SheetDocument4 pagesLife Esidimeni Fact SheetPrimedia Broadcasting100% (2)
- Full Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFDocument41 pagesFull Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFdavid.anderson198100% (37)
- Neo JaundiceDocument67 pagesNeo Jaundicemanisha thakur100% (1)
- Efolio 404Document7 pagesEfolio 404api-377789171No ratings yet
- Psychological Disorders Chapter OutlineDocument13 pagesPsychological Disorders Chapter OutlineCameron PhillipsNo ratings yet
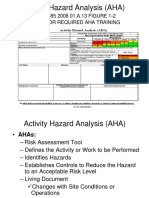
- AHA Activity Hazard AnalysisDocument24 pagesAHA Activity Hazard AnalysisElvyn Fabellore HerreraNo ratings yet
- The So Called Oedematous Skin DiseaseDocument22 pagesThe So Called Oedematous Skin Diseaseمحمد على أحمد أحمدNo ratings yet
- Health Benefits of Vitamin CDocument5 pagesHealth Benefits of Vitamin CZackNo ratings yet
- A Meningioma Is ADocument20 pagesA Meningioma Is ASherry KingNo ratings yet