You might also like
- Intravenous Vitamin CDocument3 pagesIntravenous Vitamin CnormaNo ratings yet
- DehydrationDocument17 pagesDehydrationLaura Anghel-MocanuNo ratings yet
- Filed Stamped Walgreen Erisa Complaint 8.6.19Document54 pagesFiled Stamped Walgreen Erisa Complaint 8.6.19Ann DwyerNo ratings yet
- Adult Dehydration Guideline Final 2015Document3 pagesAdult Dehydration Guideline Final 2015Brillyant S RaintamaNo ratings yet
- Dehydration Pathway 2016Document3 pagesDehydration Pathway 2016rochmandrg dokter gigiNo ratings yet
- Diabetic Ketoacidosis Protocol PICU Oct 2010 2Document9 pagesDiabetic Ketoacidosis Protocol PICU Oct 2010 2Vidini Kusuma AjiNo ratings yet
- DKA Current Practices in Africa 02 - 02 - 2022-1Document30 pagesDKA Current Practices in Africa 02 - 02 - 2022-1Raphael SeretiNo ratings yet
- (UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFDocument12 pages(UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFRizki Ismi Arsyad IINo ratings yet
- HYPO and HYPERNATREMIA IN NEONATESDocument10 pagesHYPO and HYPERNATREMIA IN NEONATESraghava mbbsNo ratings yet
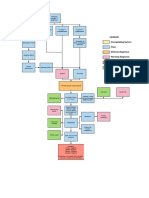
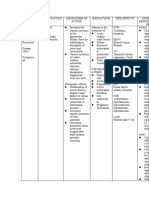
- Legend: - Precipitating Factors - Flow - Medical Diagnosis - Nursing Diagnosis - Lab Results - MedicationsDocument1 pageLegend: - Precipitating Factors - Flow - Medical Diagnosis - Nursing Diagnosis - Lab Results - MedicationsEricka GenoveNo ratings yet
- Fluid Volume Deficit (FVD)Document1 pageFluid Volume Deficit (FVD)Kathlene YuNo ratings yet
- Guidelines for treating pediatric infectious diarrheaDocument10 pagesGuidelines for treating pediatric infectious diarrheaOasis LimitedNo ratings yet
- Kuliah S2 AirDocument23 pagesKuliah S2 AirViany RehansyahNo ratings yet
- CPG Acute Infectious Diarrhea Pocket Guide v2Document21 pagesCPG Acute Infectious Diarrhea Pocket Guide v2Moonyeen Jann Casera BalicNo ratings yet
- ClinPath-10.2 - Urine and Other Body FluidsDocument4 pagesClinPath-10.2 - Urine and Other Body FluidsSanielle Karla Garcia LorenzoNo ratings yet
- GI Part 1Document3 pagesGI Part 1MaisonNo ratings yet
- Algorithm Hypertension Sci PDFDocument1 pageAlgorithm Hypertension Sci PDFGustavo CabanasNo ratings yet
- Pediatric Gastroenteritis Workup - Laboratory Studies, Imaging Studies, Other TestsDocument4 pagesPediatric Gastroenteritis Workup - Laboratory Studies, Imaging Studies, Other TestsJL CalvinNo ratings yet
- Dka AlgorithmDocument1 pageDka AlgorithmAbhinav AggarwalNo ratings yet
- Format, Drug StudyDocument23 pagesFormat, Drug StudyKrizzle Mae NeypesNo ratings yet
- University of Cebu at Pardo and Talisay, IncDocument4 pagesUniversity of Cebu at Pardo and Talisay, IncMary louicita canadaNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- Fluid and Electrolyte ImbalanceDocument18 pagesFluid and Electrolyte ImbalanceKaren PiliNo ratings yet
- Fluids and Electrolytes Study GuideDocument13 pagesFluids and Electrolytes Study GuideElizabeth McKeeNo ratings yet
- Drug Study & NCPDocument15 pagesDrug Study & NCPStephanie Mae Amoylen OdchigueNo ratings yet
- Cushing's Disease PathophysiologyDocument3 pagesCushing's Disease PathophysiologyAj MacotoNo ratings yet
- Paediatric GastroenteritisDocument6 pagesPaediatric GastroenteritisANKITA RCHAWLANo ratings yet
- Mannitol Nursing ResponsibilitiesDocument1 pageMannitol Nursing ResponsibilitiesAina HaravataNo ratings yet
- IVF Drug StudyDocument5 pagesIVF Drug StudyHannah Angelu CabadingNo ratings yet
- Drug Study-Sodium BicarbonateDocument7 pagesDrug Study-Sodium BicarbonateTrisha Faye OrtegaNo ratings yet
- Drug Study & NCPDocument12 pagesDrug Study & NCPStephanie Mae Amoylen OdchigueNo ratings yet
- Excess Fluid IntakeDocument3 pagesExcess Fluid Intakejasper pachingelNo ratings yet
- Autonomic Dysreflexia Treatment AlgorithmDocument1 pageAutonomic Dysreflexia Treatment AlgorithmdandrewmNo ratings yet
- 20-Déshydration AigueDocument4 pages20-Déshydration Aiguefatoutraore2345No ratings yet
- Renal System: Diagnostic ExaminationsDocument8 pagesRenal System: Diagnostic Examinationsjoan olanteNo ratings yet
- Cmca Assignment #3Document3 pagesCmca Assignment #3Ayanami PascuaNo ratings yet
- Mannitol Drug StudyDocument2 pagesMannitol Drug StudyNo Vem BerNo ratings yet
- Sodium Imbalances (Hyponatremia Vs Hypernatremia)Document17 pagesSodium Imbalances (Hyponatremia Vs Hypernatremia)Angel FiloteoNo ratings yet
- Electrolyte and Fluid Imbalances: Hyponatremia, Hypernatremia, HypokalemiaDocument12 pagesElectrolyte and Fluid Imbalances: Hyponatremia, Hypernatremia, HypokalemiaJuana ToriomNo ratings yet
- Analisis Laboratorium Ckd Drh FauziDocument5 pagesAnalisis Laboratorium Ckd Drh FauziachmadsahaniNo ratings yet
- TRANSF Sangre MapaDocument1 pageTRANSF Sangre MapaSiu Lin WongNo ratings yet
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- Manage side effects of osmotic diuretic mannitolDocument2 pagesManage side effects of osmotic diuretic mannitolAyesha Mae Baniaga DoctoleroNo ratings yet
- Hyperosmolar Imbalance Nursing CareDocument17 pagesHyperosmolar Imbalance Nursing CareFaye G.No ratings yet
- Antidiarrheal DrugsDocument4 pagesAntidiarrheal DrugsNadhirah ZulkifliNo ratings yet
- Diuretic types and uses explainedDocument1 pageDiuretic types and uses explainedKarinaNo ratings yet
- Drug Study TL.Document19 pagesDrug Study TL.Maria Teresa VillanuevaNo ratings yet
- Concept MapDocument1 pageConcept Mapadriana100% (1)
- Drug StudyDocument15 pagesDrug Studyjustine franchesca abonNo ratings yet
- Managing Dehydration and Electrolyte ImbalancesDocument14 pagesManaging Dehydration and Electrolyte ImbalancesAzariah EbenezerNo ratings yet
- Weak in Appearance Dry Skin Dry Mouth Decreased Urine OutputDocument5 pagesWeak in Appearance Dry Skin Dry Mouth Decreased Urine OutputromagonzalesNo ratings yet
- DengueDocument32 pagesDengueUsamaNo ratings yet
- Fluids and Electrolytes (Concentration and Composition Changes)Document6 pagesFluids and Electrolytes (Concentration and Composition Changes)Kristin SaberonNo ratings yet
- PediatricDocument10 pagesPediatrictalarashad2002No ratings yet
- Adrenal DisordersDocument1 pageAdrenal DisordersjoethemangoNo ratings yet
- GIT AgentsDocument51 pagesGIT AgentsEimhie Lee CasiNo ratings yet
- Drug StudyDocument8 pagesDrug StudyjovanneyNo ratings yet
- Pathophysiology of CholeraDocument1 pagePathophysiology of CholeraRameshKrishnanNo ratings yet
- Pathophysiology of Cholera PDFDocument1 pagePathophysiology of Cholera PDFRameshKrishnanNo ratings yet
- Drug dosage, mechanism of action, indications and nursing responsibilitiesDocument5 pagesDrug dosage, mechanism of action, indications and nursing responsibilitiesRhajeeb Aennas SugalaNo ratings yet
- Case ReportDocument13 pagesCase ReportmarselamgeNo ratings yet
- Case Report SsDocument3 pagesCase Report SsmarselamgeNo ratings yet
- Trinh 2013Document8 pagesTrinh 2013marselamgeNo ratings yet
- 10 1056@NEJMra1503884 PDFDocument10 pages10 1056@NEJMra1503884 PDFmarselamgeNo ratings yet
- AdultDehydrationGuidelineJuly2015 PDFDocument3 pagesAdultDehydrationGuidelineJuly2015 PDFmarselamgeNo ratings yet
- 28 1551 1 PBDocument6 pages28 1551 1 PBmarselamgeNo ratings yet
- Fluid MGMTDocument42 pagesFluid MGMTsakthiNo ratings yet
- Rupture SignDocument13 pagesRupture SignmarselamgeNo ratings yet
- 130-061 English 8-PagesDocument8 pages130-061 English 8-PagesmarselamgeNo ratings yet
- 10 1056@NEJMra1503884 PDFDocument10 pages10 1056@NEJMra1503884 PDFmarselamgeNo ratings yet
- Fluid MGMTDocument42 pagesFluid MGMTsakthiNo ratings yet
- 130-061 English 8-PagesDocument8 pages130-061 English 8-PagesmarselamgeNo ratings yet
- Neurogenic Bladder: When Nerve Damage Causes Bladder ProblemsDocument3 pagesNeurogenic Bladder: When Nerve Damage Causes Bladder ProblemsmarselamgeNo ratings yet
- A Rational Approach To Perioperative Fluid ManagementDocument18 pagesA Rational Approach To Perioperative Fluid ManagementmarselamgeNo ratings yet
- A Rational Approach To Perioperative Fluid ManagementDocument18 pagesA Rational Approach To Perioperative Fluid ManagementmarselamgeNo ratings yet
- 2016-BJOG An International Journal of Obstetrics & GynaecologyDocument44 pages2016-BJOG An International Journal of Obstetrics & GynaecologymarselamgeNo ratings yet
- AdultDehydrationGuidelineJuly2015 PDFDocument3 pagesAdultDehydrationGuidelineJuly2015 PDFmarselamgeNo ratings yet
- Pregnancy Tobacco PDFDocument1 pagePregnancy Tobacco PDFmarselamgeNo ratings yet
- Saving Mothers Giving Life Infographic 508ready Tag508Document2 pagesSaving Mothers Giving Life Infographic 508ready Tag508marselamgeNo ratings yet
- Aag Maternal Health PDFDocument4 pagesAag Maternal Health PDFmarselamgeNo ratings yet
- Aag Infant HealthDocument4 pagesAag Infant HealthmarselamgeNo ratings yet
- Aag Maternal Health PDFDocument4 pagesAag Maternal Health PDFmarselamgeNo ratings yet
- BS 5911-120Document33 pagesBS 5911-120Niranjan GargNo ratings yet
- Goals Editable PDFDocument140 pagesGoals Editable PDFManuel Ascanio67% (3)
- Intake Sheet SampleDocument1 pageIntake Sheet SampleRochelleNo ratings yet
- Fuck Your LawnDocument86 pagesFuck Your Lawnhuneebee100% (1)
- Position paper-MUNUCCLE 2022: Refugees) Des États !Document2 pagesPosition paper-MUNUCCLE 2022: Refugees) Des États !matNo ratings yet
- Alternate Dialysis Platforms:: Sorbents SorbentsDocument17 pagesAlternate Dialysis Platforms:: Sorbents SorbentsJoe Single100% (2)
- 4.5 Cargo DischargingDocument2 pages4.5 Cargo DischargingHasan Cosalev100% (1)
- Perforamance Based AssessmentDocument2 pagesPerforamance Based AssessmentJocelyn Acog Bisas MestizoNo ratings yet
- Workplace Hazard Analysis ProcedureDocument12 pagesWorkplace Hazard Analysis ProcedureKent Nabz60% (5)
- Puskesmas Dua Puluh Tiga Ilir Publishes Vaccination Ticket ListDocument98 pagesPuskesmas Dua Puluh Tiga Ilir Publishes Vaccination Ticket ListLaboratorium PKM 23 IlirNo ratings yet
- TDS Versimax HD4 15W40Document1 pageTDS Versimax HD4 15W40Amaraa DNo ratings yet
- Immune System Quiz ResultsDocument6 pagesImmune System Quiz ResultsShafeeq ZamanNo ratings yet
- Module A Specimen Questions January2020 PDFDocument5 pagesModule A Specimen Questions January2020 PDFShashi Bhusan SinghNo ratings yet
- Quality ImprovementDocument3 pagesQuality ImprovementViky SinghNo ratings yet
- Stress and FilipinosDocument28 pagesStress and FilipinosDaniel John Arboleda100% (2)
- Maual de Servicio TV LG 32lf15r-MaDocument31 pagesMaual de Servicio TV LG 32lf15r-MaJaime E FernandezNo ratings yet
- Exercise 4 Summary - KEY PDFDocument3 pagesExercise 4 Summary - KEY PDFFrida Olea100% (1)
- Válvulas Flomatic USADocument40 pagesVálvulas Flomatic USAEfrain DuarteNo ratings yet
- Rapid Cycling in Bipolar DisorderDocument1 pageRapid Cycling in Bipolar Disorderdo leeNo ratings yet
- WSAWLD002Document29 pagesWSAWLD002Nc BeanNo ratings yet
- Elem. Reading PracticeDocument10 pagesElem. Reading PracticeElissa Janquil RussellNo ratings yet
- Human Capital FormationDocument9 pagesHuman Capital Formationtannu singh67% (6)
- Jairo Garzon 1016001932 G900003 1580 Task4Document12 pagesJairo Garzon 1016001932 G900003 1580 Task4Jairo Garzon santanaNo ratings yet
- Scaffolding Control & MeasuresDocument3 pagesScaffolding Control & Measuresviswamanoj100% (1)
- Hydrogeological Characterization of Karst Areas in NW VietnamDocument152 pagesHydrogeological Characterization of Karst Areas in NW VietnamCae Martins100% (1)
- Spec BoilerDocument9 pagesSpec BoilerAchmad MakmuriNo ratings yet
- A&P 2 - Digestive System Flashcards - QuizletDocument1 pageA&P 2 - Digestive System Flashcards - QuizletMunachande KanondoNo ratings yet
- Magnetic FieldDocument19 pagesMagnetic FieldNitinSrivastava100% (2)
- New930e-4se Ceam031503 930e4se Omm A31937 Up PDFDocument273 pagesNew930e-4se Ceam031503 930e4se Omm A31937 Up PDFSergelen SakhyabazarNo ratings yet
- Aphasia PDFDocument4 pagesAphasia PDFRehab Wahsh100% (1)