You might also like
- Journal Medicine: The New EnglandDocument9 pagesJournal Medicine: The New EnglandFernanda Araújo AvendanhaNo ratings yet
- Womenshealth & NutritionDocument5 pagesWomenshealth & Nutritionbragaru.vladNo ratings yet
- Causes of Changes in Carotid Intima-Media Thickness: A Literature ReviewDocument10 pagesCauses of Changes in Carotid Intima-Media Thickness: A Literature ReviewSorin ParalescuNo ratings yet
- Trends in Cardiovascular Health Metrics in Obese Adults: National Health and Nutrition Examination Survey (NHANES), 1988 - 2014Document20 pagesTrends in Cardiovascular Health Metrics in Obese Adults: National Health and Nutrition Examination Survey (NHANES), 1988 - 2014Desy YardinaNo ratings yet
- Primary and Secondary Prevention of Coronary Artery DiseaseDocument24 pagesPrimary and Secondary Prevention of Coronary Artery DiseaseNatalia GeofaniNo ratings yet
- Primary and Secondary Prevention of Coronary Artery Disease - Overview, Risk AsseDocument32 pagesPrimary and Secondary Prevention of Coronary Artery Disease - Overview, Risk Asseליסה לרנרNo ratings yet
- Dose-Response Association of Uncontrolled Blood Pressure and Cardiovascular Disease Risk Factors With Hyperuricemia and GoutDocument8 pagesDose-Response Association of Uncontrolled Blood Pressure and Cardiovascular Disease Risk Factors With Hyperuricemia and GoutxoxotheNo ratings yet
- ANNALS DyslipidemiaDocument16 pagesANNALS Dyslipidemiaewb100% (1)
- Cuadro de Horarios Paa RellenarDocument7 pagesCuadro de Horarios Paa RellenarLuis ChangaNo ratings yet
- Thừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardDocument24 pagesThừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardNam NguyenHoangNo ratings yet
- Serum Alpha-Carotene Concentrations and Risk of Death Among US AdultsDocument9 pagesSerum Alpha-Carotene Concentrations and Risk of Death Among US AdultsCherry San DiegoNo ratings yet
- Stoke NutritionDocument14 pagesStoke Nutritionapi-150223943No ratings yet
- Dyson LineDocument10 pagesDyson LineSharly DwijayantiNo ratings yet
- Final Research ProjectDocument21 pagesFinal Research Projectapi-339312954No ratings yet
- Ni Hms 366201Document17 pagesNi Hms 366201Habiburrahman EffendyNo ratings yet
- Diagnosis of Early Risks, Management of Risks, and Reduction of Vascular DiseasesDocument11 pagesDiagnosis of Early Risks, Management of Risks, and Reduction of Vascular DiseasesasclepiuspdfsNo ratings yet
- Harmonizing The Metabolic SyndromeDocument7 pagesHarmonizing The Metabolic SyndromeCarlos_RuedasNo ratings yet
- IV Abra DineDocument13 pagesIV Abra DinelilisNo ratings yet
- Review ArticleDocument14 pagesReview ArticlePanji Agung KhrisnaNo ratings yet
- Andrew Maxwell, M.D.: From: Sent: To: SubjectDocument4 pagesAndrew Maxwell, M.D.: From: Sent: To: SubjectHeart of the Valley, Pediatric CardiologyNo ratings yet
- Hypercholesterolemia Among Children: When Is It High, and When Is It Really High?Document4 pagesHypercholesterolemia Among Children: When Is It High, and When Is It Really High?Brenda CaraveoNo ratings yet
- The Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeDocument7 pagesThe Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeEmir SaricNo ratings yet
- Novel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research AnDocument8 pagesNovel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research Analerta.bfcmNo ratings yet
- Hypertension in PregnancyDocument5 pagesHypertension in PregnancyLalita Eka Pervita SariNo ratings yet
- Ahei & HeiDocument12 pagesAhei & HeiBushra KainaatNo ratings yet
- Artikel 4 - CohortDocument9 pagesArtikel 4 - Cohort048Auliatur RohmahNo ratings yet
- Assessment of College Students Awareness and Knowledge About Conditions Relevant To Metabolic SyndromeDocument15 pagesAssessment of College Students Awareness and Knowledge About Conditions Relevant To Metabolic SyndromeManimegalai SNo ratings yet
- Background of The StudyDocument10 pagesBackground of The StudyReimond VinceNo ratings yet
- What Is A Cardiovascular Risk and Factors?Document7 pagesWhat Is A Cardiovascular Risk and Factors?Rahul SharmaNo ratings yet
- Hostility and The Metabolic Syndrome in Older Males: The Normative Aging StudyDocument10 pagesHostility and The Metabolic Syndrome in Older Males: The Normative Aging StudymrclpppNo ratings yet
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030No ratings yet
- Raman, G 2019Document12 pagesRaman, G 2019Nicolás MurilloNo ratings yet
- AHA/ADA Scientific StatementDocument29 pagesAHA/ADA Scientific StatementpukpigjNo ratings yet
- Diabetes Hypertension Obesity: PathophysiologyDocument3 pagesDiabetes Hypertension Obesity: PathophysiologyDevy AndikaNo ratings yet
- The Impact of Egg Limitations On CHD PDFDocument9 pagesThe Impact of Egg Limitations On CHD PDFAndri NugrahaNo ratings yet
- Healthy Lifestyle and The Risk of Stroke in Women: BackgroundDocument11 pagesHealthy Lifestyle and The Risk of Stroke in Women: BackgroundGlaiza CzarinaNo ratings yet
- Medical Tribune May 2013Document39 pagesMedical Tribune May 2013Marissa WreksoatmodjoNo ratings yet
- VITAMINA D y Riesgo CardiovascularDocument12 pagesVITAMINA D y Riesgo CardiovascularAngusNo ratings yet
- CA Cancer J ClinDocument29 pagesCA Cancer J ClinanshunigamNo ratings yet
- Polygenic Hypercholesterolemia: Causes, Risks & TreatmentDocument6 pagesPolygenic Hypercholesterolemia: Causes, Risks & TreatmentSamhitha Ayurvedic ChennaiNo ratings yet
- 4 - Health Consequences of Obesity 2012Document5 pages4 - Health Consequences of Obesity 2012Mateus CarvalhoNo ratings yet
- AbstractDocument1 pageAbstractmich__aishkaiNo ratings yet
- PIIS0002934311002920 CGHDocument10 pagesPIIS0002934311002920 CGHJulianda Dini HalimNo ratings yet
- Cost-Effectiveness of Hypertension Therapy According To 2014 GuidelinesDocument9 pagesCost-Effectiveness of Hypertension Therapy According To 2014 GuidelinesIsti YaniNo ratings yet
- Https/www-Uptodate-Com Consultaremota Upb Edu Co/contents/management-Of-CDocument34 pagesHttps/www-Uptodate-Com Consultaremota Upb Edu Co/contents/management-Of-CMichael Amarillo CorreaNo ratings yet
- Nutrients: Dietary Interventions For Gout and E Cardiovascular Risk Factors: A Systematic ReviewDocument19 pagesNutrients: Dietary Interventions For Gout and E Cardiovascular Risk Factors: A Systematic ReviewVika NovikaNo ratings yet
- Science Fair Final ReportDocument16 pagesScience Fair Final ReportNishorgo SarkarNo ratings yet
- Modified Mediterranean Diet Score and Cardiovascular Risk in A North American Working PopulationDocument10 pagesModified Mediterranean Diet Score and Cardiovascular Risk in A North American Working Populationapi-356847931No ratings yet
- Gastroenteritis Outbreak Tied To Later Health Problems: HealthdayDocument5 pagesGastroenteritis Outbreak Tied To Later Health Problems: HealthdayJammae RubillosNo ratings yet
- NAFLDDocument17 pagesNAFLDJirran CabatinganNo ratings yet
- Zalesin 2008Document22 pagesZalesin 2008Dinti wardaNo ratings yet
- 2019 ACC - AHA Guideline On The Primary Prevention of Cardiovascular Disease - American College of CardiologyDocument9 pages2019 ACC - AHA Guideline On The Primary Prevention of Cardiovascular Disease - American College of CardiologyYasinta FebrianaNo ratings yet
- ACS Guidelines PDFDocument38 pagesACS Guidelines PDFGabriel MateusNo ratings yet
- 6.vol5 Issue2 2017 MS 15392Document4 pages6.vol5 Issue2 2017 MS 15392iamsleepless007No ratings yet
- Cardiometabolic Syndrome PipinDocument15 pagesCardiometabolic Syndrome Pipinspider_mechNo ratings yet
- Evidence Based Cardiology 4th EdDocument424 pagesEvidence Based Cardiology 4th EdROGER LUDEÑA SALAZARNo ratings yet
- 2017, Guerra-Silva IJCDocument7 pages2017, Guerra-Silva IJCNatalia Maria Maciel GuerraNo ratings yet
- Medical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660Document6 pagesMedical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660David WheelerNo ratings yet
- nutrients-10-01385Document16 pagesnutrients-10-01385Alex GutiérrezNo ratings yet
- Daftar Dosis Dan Sediaan ObatDocument5 pagesDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- Drug Doses 2017Document127 pagesDrug Doses 2017Yuliawati HarunaNo ratings yet
- Daftar Dosis Dan Sediaan ObatDocument5 pagesDaftar Dosis Dan Sediaan ObatVenessa Rudy Pranata97% (38)
- Westeergard Focus On Abnormal Air PDFDocument8 pagesWesteergard Focus On Abnormal Air PDFIndah RismandasariNo ratings yet
- CR 07 167Document6 pagesCR 07 167Indah RismandasariNo ratings yet
- Book 1Document2 pagesBook 1Indah RismandasariNo ratings yet
- Ojog 2016042617575247Document7 pagesOjog 2016042617575247Mahdiah JabailusNo ratings yet
- WikiAbdominal Pain PDFDocument6 pagesWikiAbdominal Pain PDFIndah RismandasariNo ratings yet
- DR P Nel The Diagnostic Role of Sonar and CT-scan inDocument21 pagesDR P Nel The Diagnostic Role of Sonar and CT-scan inIndah RismandasariNo ratings yet
- Acute Abdomen Pre and Post-Laparotomy DiagnosisDocument10 pagesAcute Abdomen Pre and Post-Laparotomy DiagnosisIndah RismandasariNo ratings yet
- Heart: Yvan Patrick AkréDocument1 pageHeart: Yvan Patrick AkréIndah RismandasariNo ratings yet
- Poster52 PDFDocument1 pagePoster52 PDFIndah RismandasariNo ratings yet
- 2016 Article 291Document4 pages2016 Article 291Indah RismandasariNo ratings yet
- HPV 180Document9 pagesHPV 180Indah RismandasariNo ratings yet
- E003682 FullDocument13 pagesE003682 FullIndah RismandasariNo ratings yet
- Sepsis N Endothelial PermeabilityDocument3 pagesSepsis N Endothelial PermeabilityIndah RismandasariNo ratings yet
- E004758 FullDocument11 pagesE004758 FullIndah RismandasariNo ratings yet
- 2017 Article 482Document8 pages2017 Article 482Indah RismandasariNo ratings yet
- CHT Acfa Boys Z 3 5Document1 pageCHT Acfa Boys Z 3 5Rivadin NurwanNo ratings yet
- 2016 Article 442Document8 pages2016 Article 442Indah RismandasariNo ratings yet
- 2016 Article 189Document12 pages2016 Article 189Indah RismandasariNo ratings yet
- 2017 Article 478Document10 pages2017 Article 478Indah RismandasariNo ratings yet
- Liquorice: A Root Cause of Secondary Hypertension: Ravi Varma and Calum N. RossDocument3 pagesLiquorice: A Root Cause of Secondary Hypertension: Ravi Varma and Calum N. RossIndah RismandasariNo ratings yet
- Z Scores PDFDocument29 pagesZ Scores PDFIndah RismandasariNo ratings yet
- CHT Acfa Boys Z 3 5Document1 pageCHT Acfa Boys Z 3 5Rivadin NurwanNo ratings yet
- ABC of BurnDocument3 pagesABC of BurnJokevin PrasetyadhiNo ratings yet
- WHO Grow Chart TB+U Girl 5-19Document1 pageWHO Grow Chart TB+U Girl 5-19Kartika AnggakusumaNo ratings yet
- BMJ BurnDocument3 pagesBMJ BurnNila SariNo ratings yet
- WikiAbdominal PainDocument6 pagesWikiAbdominal PainIndah RismandasariNo ratings yet
- Acute Abdominal Emergencies GuideDocument126 pagesAcute Abdominal Emergencies GuidekityamuwesiNo ratings yet
- Naming, Labeling, and Packaging of Pharmaceuticals: Special FeaturesDocument9 pagesNaming, Labeling, and Packaging of Pharmaceuticals: Special FeaturesjovanaNo ratings yet
- Methodical Instructions: For The Practical Classes in Pharmacology TopicDocument3 pagesMethodical Instructions: For The Practical Classes in Pharmacology TopicSahil SainiNo ratings yet
- Diagnosing Secondary and Primary Headache Disorders: Review ArticleDocument14 pagesDiagnosing Secondary and Primary Headache Disorders: Review ArticleMD IurieNo ratings yet
- Hiperakusis 2015Document20 pagesHiperakusis 2015Abdur ShamilNo ratings yet
- TeratologyDocument36 pagesTeratologySafera RezaNo ratings yet
- Training Design AprilDocument3 pagesTraining Design AprilZed P. EstalillaNo ratings yet
- Quality of life and insomnia treatmentDocument14 pagesQuality of life and insomnia treatmentAkhmad VauwazNo ratings yet
- First Aid Manual Rev 0Document77 pagesFirst Aid Manual Rev 0Vinayak KaujalgiNo ratings yet
- Psychiatric History and Mental Status ExamDocument81 pagesPsychiatric History and Mental Status ExamErsido SamuelNo ratings yet
- Assessment ToolDocument13 pagesAssessment Toolal gulNo ratings yet
- KARDEX Case 1Document3 pagesKARDEX Case 1Juviely PremacioNo ratings yet
- Renal Failure and ItsDocument8 pagesRenal Failure and ItsSandra CalderonNo ratings yet
- Aapm TG 179Document18 pagesAapm TG 179Ahmet Kürşat ÖzkanNo ratings yet
- Clinical PathwayDocument91 pagesClinical PathwaytiganovNo ratings yet
- Fendo 13 967102Document9 pagesFendo 13 967102Vilma Gladis Rios HilarioNo ratings yet
- ShiatsuDocument20 pagesShiatsuMarko Ranitovic100% (1)
- Abnormal Psychology TestDocument7 pagesAbnormal Psychology TestCamae Snyder GangcuangcoNo ratings yet
- Internship 3Document4 pagesInternship 3Hirschmann Andro BoquilaNo ratings yet
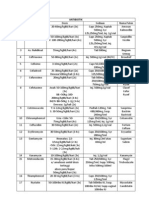
- NASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikDocument1 pageNASYTA DIFA FIRDAUS - Tabel Pengelompokkan AntibiotikNasyta Difa FirdausNo ratings yet
- 2 MergedDocument11 pages2 MergedMudasir ElahiNo ratings yet
- Smiths Medical Cadd Legacy Pca 6300 User Manual PDFDocument102 pagesSmiths Medical Cadd Legacy Pca 6300 User Manual PDFJr BraduNo ratings yet
- Heart Defects and Vascular Anomalies: Causes, Types and TreatmentDocument17 pagesHeart Defects and Vascular Anomalies: Causes, Types and TreatmentA.V.M.No ratings yet
- Bala MedicinalDocument23 pagesBala MedicinalJayesh BoroleNo ratings yet
- Wcet2016 Programme and Abstract BookDocument64 pagesWcet2016 Programme and Abstract BookMohyuddin A MaroofNo ratings yet
- Vaccine: Contents Lists Available atDocument9 pagesVaccine: Contents Lists Available atShabrina Amalia SuciNo ratings yet
- Respiratory FailureDocument8 pagesRespiratory FailureAnusha VergheseNo ratings yet
- CMC HIS User Manual SummaryDocument40 pagesCMC HIS User Manual Summarymanotiwa0% (1)
- Uterine Prolapse CaseDocument23 pagesUterine Prolapse CaseJonathan GnwNo ratings yet
- Basic of Ot 1Document2 pagesBasic of Ot 1shubham vermaNo ratings yet