You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Personality in Organizations - LO3Document8 pagesPersonality in Organizations - LO3Nicasio AquinoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Supply Chain Supply Chain ManagementDocument1 pageSupply Chain Supply Chain ManagementNicasio AquinoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
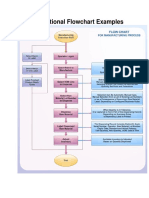
- Flowchart of Work Flow Document For A Manufacturing CompanyDocument2 pagesFlowchart of Work Flow Document For A Manufacturing CompanyNicasio AquinoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Air Asia 3Document5 pagesAir Asia 3Nicasio AquinoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Software Engineering Interview QuestionsDocument8 pagesSoftware Engineering Interview QuestionsNicasio AquinoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Vision Statement Should Answer The Basic Question, "What Do We Want To Become?"Document12 pagesA Vision Statement Should Answer The Basic Question, "What Do We Want To Become?"Nicasio AquinoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Inventory Management Process FlowchartDocument5 pagesInventory Management Process FlowchartNicasio AquinoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- SAP End To EndDocument18 pagesSAP End To EndNicasio AquinoNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Computer Forensics Final GradeDocument15 pagesComputer Forensics Final GradeNicasio AquinoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Inventory System X Functional FlowchartDocument1 pageInventory System X Functional FlowchartNicasio AquinoNo ratings yet
- Title - TRAIN Law and Other Tax Updates BookeepingDocument2 pagesTitle - TRAIN Law and Other Tax Updates BookeepingNicasio AquinoNo ratings yet
- Research 11 Writing GuidelinesDocument3 pagesResearch 11 Writing GuidelinesNicasio AquinoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 1 Race 2 End WasteDocument6 pages1 Race 2 End WasteNicasio AquinoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Credit Risk Management-1Document74 pagesCredit Risk Management-1Nicasio AquinoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- CPA Review: Code of Ethics for Professional Accountants in the PhilippinesDocument20 pagesCPA Review: Code of Ethics for Professional Accountants in the PhilippinesJedidiah SmithNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Test of Controls Procedure PDFDocument6 pagesTest of Controls Procedure PDFNatsu DragneelNo ratings yet
- Corporate LiquidationDocument7 pagesCorporate LiquidationNathallie CabalunaNo ratings yet
- Enactus Case StudyDocument10 pagesEnactus Case StudyNicasio AquinoNo ratings yet
- Forensic NicsDocument12 pagesForensic NicsNicasio AquinoNo ratings yet
- Carl Von ClausewitzDocument7 pagesCarl Von ClausewitzNicasio AquinoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Guide RFP WritingDocument3 pagesGuide RFP WritingSunilBhandari100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Dietary Fats and Cardiovascular DiseaseDocument25 pagesDietary Fats and Cardiovascular DiseaseNicasio AquinoNo ratings yet
- What Is Artificial Intelligence - by Raymond de LacazeDocument22 pagesWhat Is Artificial Intelligence - by Raymond de LacazeNicasio AquinoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Venezuela Goes Bust - WSJDocument2 pagesVenezuela Goes Bust - WSJNicasio AquinoNo ratings yet
- Injecting Virus Into Brain May Relieve Parkinson's Symptoms - New ScientistDocument2 pagesInjecting Virus Into Brain May Relieve Parkinson's Symptoms - New ScientistNicasio AquinoNo ratings yet
- 1b. Writing Terms of Reference For An EvaluationDocument32 pages1b. Writing Terms of Reference For An EvaluationAle CevallosNo ratings yet
- Shotokan's Secret QuoteDocument1 pageShotokan's Secret QuoteNicasio AquinoNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Business Law 1Document25 pagesBusiness Law 1Nicasio AquinoNo ratings yet
- You Can't Understand ISIS If You Don't Know The History of Wahhabism in Saudi ArabiaDocument17 pagesYou Can't Understand ISIS If You Don't Know The History of Wahhabism in Saudi ArabiaNicasio AquinoNo ratings yet
- Registration Procedure of Marketing Authorization of Medicinal Product in MalaysiaDocument17 pagesRegistration Procedure of Marketing Authorization of Medicinal Product in MalaysiaFitrah Zulfikar MansyurNo ratings yet
- Short Listed BooksDocument3 pagesShort Listed BooksWaseem HaiderNo ratings yet
- Introduction To Clinical ResearchDocument19 pagesIntroduction To Clinical ResearchVignesh GaneshNo ratings yet
- Daftar Inventaris Buku FFDocument71 pagesDaftar Inventaris Buku FFcakra gilingNo ratings yet
- Module 2 - Regulatory Approval Process - Lecture NotesDocument16 pagesModule 2 - Regulatory Approval Process - Lecture NotesyvssmanjunathNo ratings yet
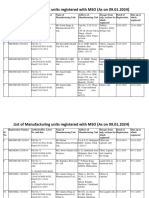
- MSO Latest - Manufacturing - Unit - 12Document46 pagesMSO Latest - Manufacturing - Unit - 12sunshine7883No ratings yet
- Pharmacist Licensing Exam ReferencesDocument2 pagesPharmacist Licensing Exam ReferencesAnas KtNo ratings yet
- New Drug Development and Approval ProcessDocument152 pagesNew Drug Development and Approval ProcessJhef ebuengaNo ratings yet
- Pharmacology NotesDocument2 pagesPharmacology Notessakuragi jakeNo ratings yet
- Appendix C2 Cover Letter ASUBARDocument2 pagesAppendix C2 Cover Letter ASUBARRuel Vincent AsubarNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Jurnal Epo 1Document7 pagesJurnal Epo 1Evelin VelinnNo ratings yet
- Handbook of Pharmaceutical BiotechnologyDocument6 pagesHandbook of Pharmaceutical Biotechnologymc2camilaNo ratings yet
- Orphan DrugsDocument14 pagesOrphan DrugsLeah BralowNo ratings yet
- ICH M13A Webinar Slides May 2023Document55 pagesICH M13A Webinar Slides May 2023Miy AichNo ratings yet
- The Establishment of Emerging Trial RegionsDocument44 pagesThe Establishment of Emerging Trial Regionsmshankar230% (1)
- MCQ 1 General Introduction and PharmacokineticsDocument7 pagesMCQ 1 General Introduction and PharmacokineticsVarmaNo ratings yet
- (Doi 10.1016/j.ijpharm.2015.01.022) T. Loftsson - Excipient Pharmacokinetics and ProfilingDocument7 pages(Doi 10.1016/j.ijpharm.2015.01.022) T. Loftsson - Excipient Pharmacokinetics and ProfilingRia DeviNo ratings yet
- Aps Uk Pharm Sci Poster 2014 PDFDocument1 pageAps Uk Pharm Sci Poster 2014 PDFapi-266268510No ratings yet
- Form Gyssens (PASIEN 1)Document9 pagesForm Gyssens (PASIEN 1)Wahyu NugraheniNo ratings yet
- Quintus SlidesCarnivalDocument103 pagesQuintus SlidesCarnivalmiles sbNo ratings yet
- Gowthami - BIO Jr. Research Associate - 3+ Yrs Exp - ProfileDocument4 pagesGowthami - BIO Jr. Research Associate - 3+ Yrs Exp - ProfileMuraliNaiduNo ratings yet
- Clinical Trials in A Nut ShellDocument23 pagesClinical Trials in A Nut ShellSuryamohan SurampudiNo ratings yet
- MMMDocument4 pagesMMMRamaSaputriKuzanNo ratings yet
- Clinical Protocol by EktaDocument24 pagesClinical Protocol by EktaEkta SharmaNo ratings yet
- FAESGraduateSchoolAtNIH2014 2015Document124 pagesFAESGraduateSchoolAtNIH2014 2015Anonymous hK9rR30No ratings yet
- Introduction To Clinical ResearchDocument19 pagesIntroduction To Clinical ResearchVignesh GaneshNo ratings yet
- Lecture Slides-Cvt Lec0b Charron CourseraDocument16 pagesLecture Slides-Cvt Lec0b Charron Courseratamara_0021No ratings yet
- Declaration of HelsinkiDocument11 pagesDeclaration of HelsinkiYzel Vasquez AdavanNo ratings yet
- Medication Pathway (Prescription) PDFDocument162 pagesMedication Pathway (Prescription) PDFChristine Annmarie TapawanNo ratings yet
- Stockleys 12e - 9780857113474 PDFDocument1 pageStockleys 12e - 9780857113474 PDFPark arimaNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceFrom EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceRating: 4.5 out of 5 stars4.5/5 (515)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsFrom EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsRating: 4.5 out of 5 stars4.5/5 (4)
- This Is Your Brain On Parasites: How Tiny Creatures Manipulate Our Behavior and Shape SocietyFrom EverandThis Is Your Brain On Parasites: How Tiny Creatures Manipulate Our Behavior and Shape SocietyRating: 3.5 out of 5 stars3.5/5 (31)
- The Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorFrom EverandThe Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorNo ratings yet
- The Consciousness Instinct: Unraveling the Mystery of How the Brain Makes the MindFrom EverandThe Consciousness Instinct: Unraveling the Mystery of How the Brain Makes the MindRating: 4.5 out of 5 stars4.5/5 (93)
- Crypt: Life, Death and Disease in the Middle Ages and BeyondFrom EverandCrypt: Life, Death and Disease in the Middle Ages and BeyondRating: 4 out of 5 stars4/5 (3)