You might also like
- Visual Mnemonics Medicine 2e 40 Medical Mnemonics 41 40 Oct 16 2019 41 40 1700212737 41 40 Independently Published 41Document146 pagesVisual Mnemonics Medicine 2e 40 Medical Mnemonics 41 40 Oct 16 2019 41 40 1700212737 41 40 Independently Published 41El Farouk100% (1)
- Seagate Part1 PDFDocument113 pagesSeagate Part1 PDFwaranhaNo ratings yet
- Modern Scoring BRASS Manual1Document25 pagesModern Scoring BRASS Manual1Pepe ChorrasNo ratings yet
- Renal Cell Carcinoma Risk Factors & TypesDocument1 pageRenal Cell Carcinoma Risk Factors & TypesBobet ReñaNo ratings yet
- Colorectal CancerDocument8 pagesColorectal Cancerjorgeacct100% (3)
- Circulation Study Guide Chapters 14-24Document3 pagesCirculation Study Guide Chapters 14-24raanja2No ratings yet
- Paroxysmal Nocturnal Hemoglobinuria Case StudyDocument87 pagesParoxysmal Nocturnal Hemoglobinuria Case Studyrachael100% (4)
- Manual Handbook Ripping Cat Selection Techniques Applications Production CompatibilityDocument32 pagesManual Handbook Ripping Cat Selection Techniques Applications Production CompatibilityPoPandaNo ratings yet
- Lectures Note Parasitology FinalDocument284 pagesLectures Note Parasitology FinalEl Farouk100% (2)
- Well CompletionDocument26 pagesWell Completionnitesh kumarNo ratings yet
- Introduction To Probability: Business Statistics: Communicating With Numbers, 4eDocument52 pagesIntroduction To Probability: Business Statistics: Communicating With Numbers, 4eRetno Ajeng Anissa WidiatriNo ratings yet
- Paraneoplastic syndromes in lung cancerDocument35 pagesParaneoplastic syndromes in lung cancerEl FaroukNo ratings yet
- Colorectal CancerDocument18 pagesColorectal CancerKimie PanganNo ratings yet
- Case StudyDocument21 pagesCase StudyLuige AvilaNo ratings yet
- First Quarter - Curriculum Map - Science 8Document7 pagesFirst Quarter - Curriculum Map - Science 8Mich Hora100% (7)
- Goju Ryu TerminologyDocument14 pagesGoju Ryu TerminologyProbeer123No ratings yet
- Goju Ryu TerminologyDocument14 pagesGoju Ryu TerminologyProbeer123No ratings yet
- Colorectal CancerDocument3 pagesColorectal CancerAriane May Rubio50% (2)
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisNo ratings yet
- Health Education ProgramDocument4 pagesHealth Education ProgramZari Novela100% (1)
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayNo ratings yet
- Cancer Prevention, Screening, & Early DetectionDocument13 pagesCancer Prevention, Screening, & Early Detectionchfalguera100% (1)
- Pancreatic Cancer: Early Detection Offers Best Chance of CureDocument18 pagesPancreatic Cancer: Early Detection Offers Best Chance of Curemywifenoor1983No ratings yet
- MelanomaDocument14 pagesMelanomaMarco Antonio Koff100% (1)
- Malignant MelanomaDocument31 pagesMalignant MelanomakityamuwesiNo ratings yet
- Tumor marker classification and applicationsDocument30 pagesTumor marker classification and applicationsnouval_iqbal100% (1)
- B. Pathophysiology: Clinical Aspects of Cancer DiagnosisDocument10 pagesB. Pathophysiology: Clinical Aspects of Cancer DiagnosisAbigael Patricia GutierrezNo ratings yet
- Smart AntennasDocument40 pagesSmart AntennasMeeraNo ratings yet
- Seminar ON Peptic Ulcer: Presented By: Ms. Sweta SinghDocument26 pagesSeminar ON Peptic Ulcer: Presented By: Ms. Sweta Singhshweta singhNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Cocoa Fermentation ManualDocument18 pagesCocoa Fermentation ManualJimena Rios100% (1)
- Case Study Endometrial PDFDocument17 pagesCase Study Endometrial PDFapi-279886264No ratings yet
- Zollinger-Ellison Syndrome (Gastrinoma)Document15 pagesZollinger-Ellison Syndrome (Gastrinoma)Huy QuangNo ratings yet
- Control Yokogawa PDFDocument59 pagesControl Yokogawa PDFmiraNo ratings yet
- Colon CancerDocument65 pagesColon CancerKristine Young100% (1)
- Gastric CarcinomaDocument21 pagesGastric CarcinomaAli Abbas100% (2)
- Prevention & Detection of CANCERDocument32 pagesPrevention & Detection of CANCERSiddharth JainNo ratings yet
- Gastric CancerDocument7 pagesGastric CancerMicah PingawanNo ratings yet
- Cancer PathophysiologyDocument10 pagesCancer PathophysiologyGia Bautista-AmbasingNo ratings yet
- Case Analysis Group 1Document47 pagesCase Analysis Group 1bunso padillaNo ratings yet
- Breast Cancer Case Study: Answers For LifeDocument4 pagesBreast Cancer Case Study: Answers For LifeFaye Mie VelascoNo ratings yet
- Systemic Lupus Erythematosus (SLE)Document39 pagesSystemic Lupus Erythematosus (SLE)Nadya SabrinaNo ratings yet
- Treatments and Drugs: by Mayo Clinic StaffDocument23 pagesTreatments and Drugs: by Mayo Clinic StaffJr D BayzNo ratings yet
- Phyllodes Tumors of The Breast UpToDateDocument22 pagesPhyllodes Tumors of The Breast UpToDateSean SialanaNo ratings yet
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- Prostate Cancer: Signs and SymptomsDocument5 pagesProstate Cancer: Signs and SymptomsLicio LentimoNo ratings yet
- Systemic Lupus ErythematosusDocument37 pagesSystemic Lupus ErythematosusFirman Ichlasul AmalNo ratings yet
- Understanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentDocument3 pagesUnderstanding Hepatic Encephalopathy (HE) Symptoms, Causes and TreatmentSuhas KandeNo ratings yet
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocument22 pagesManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNo ratings yet
- Acute Liver Failure in ChildrenDocument34 pagesAcute Liver Failure in ChildrenEpahNo ratings yet
- Cancer Prevention Health Education ProgramDocument9 pagesCancer Prevention Health Education ProgramKheneille Vaughn Javier GuevarraNo ratings yet
- Cancer of The ColonDocument8 pagesCancer of The Colonnot your medz duranNo ratings yet
- Breast Cancer SukumarDocument85 pagesBreast Cancer SukumarPrima MedikaNo ratings yet
- Nursing Process OsteosarcomaDocument34 pagesNursing Process OsteosarcomaDonJohnNo ratings yet
- Case Presentation TetanusDocument15 pagesCase Presentation TetanusukhtianitaNo ratings yet
- Liver CancerDocument2 pagesLiver CancerPrincess Barnuevo100% (2)
- Systemic Lupus ErythematosusDocument46 pagesSystemic Lupus ErythematosuspriscillaNo ratings yet
- Stomach CancerDocument7 pagesStomach CancerSyazmin KhairuddinNo ratings yet
- A Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeDocument3 pagesA Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeIOSRjournalNo ratings yet
- Gastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDocument31 pagesGastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDeep KhemaniNo ratings yet
- Diverticular DiseaseDocument15 pagesDiverticular DiseaseRogie SaludoNo ratings yet
- Kay - OR CaseDocument9 pagesKay - OR CaseSienaNo ratings yet
- PericarditisDocument11 pagesPericarditisrbarcellonaNo ratings yet
- Acute Lymphocytic LeukemiaDocument12 pagesAcute Lymphocytic Leukemiajustin_saneNo ratings yet
- Bladder CancerDocument35 pagesBladder CancerHealth Education Library for PeopleNo ratings yet
- The Following List Illustrates The Content of A Complete Review of SystemsDocument1 pageThe Following List Illustrates The Content of A Complete Review of SystemsHazel CastorNo ratings yet
- CASE STUDY: B-ALL WITH APLASTIC ANEMIADocument15 pagesCASE STUDY: B-ALL WITH APLASTIC ANEMIAShakira HashimNo ratings yet
- Breast Cancer (Research Paper)Document12 pagesBreast Cancer (Research Paper)Katrina Arnaiz100% (3)
- Day 2 - Ulcerative Colitis PDFDocument14 pagesDay 2 - Ulcerative Colitis PDFMaria Charis Anne IndananNo ratings yet
- Congenital Heart DiseaseDocument12 pagesCongenital Heart Diseaserakanootousan100% (1)
- Chemotherapy - Alkylating AgentsDocument33 pagesChemotherapy - Alkylating AgentsNolan100% (1)
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathyAnonymous GIGXKjfLNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
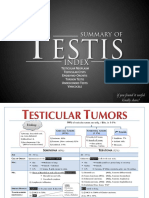
- Testis SummaryDocument10 pagesTestis SummaryEl FaroukNo ratings yet
- Mscsurgicalskillspt 20211003Document3 pagesMscsurgicalskillspt 20211003El FaroukNo ratings yet
- Atlas CardiologieDocument143 pagesAtlas CardiologieEl FaroukNo ratings yet
- ترجمه أسئله اختبار الكوميتيه 2018Document17 pagesترجمه أسئله اختبار الكوميتيه 2018El FaroukNo ratings yet
- PharmacologyDocument102 pagesPharmacologyAbrar SabawiNo ratings yet
- PharmacologyDocument102 pagesPharmacologyAbrar SabawiNo ratings yet
- DASH Diet Cookbook - Quick and E - Dylanna PressDocument113 pagesDASH Diet Cookbook - Quick and E - Dylanna PressEl FaroukNo ratings yet
- Neurosurgery Summaryupdated PDFDocument16 pagesNeurosurgery Summaryupdated PDFEl FaroukNo ratings yet
- Lecture notes on human respiratory system physiologyDocument33 pagesLecture notes on human respiratory system physiologyMiles HuiNo ratings yet
- Comprehensive Table of Drugs: Cholinergic Agonists (Parasympathomimetics)Document31 pagesComprehensive Table of Drugs: Cholinergic Agonists (Parasympathomimetics)filchibuffNo ratings yet
- ترجمه اختبار الكاتا 2018 1Document10 pagesترجمه اختبار الكاتا 2018 1El FaroukNo ratings yet
- Lect 75control of Tissue Blood FlowDocument23 pagesLect 75control of Tissue Blood FlowEl FaroukNo ratings yet
- Key Concepts:: For Information or Comments On This Tutorial, Please Contact R. Frey atDocument12 pagesKey Concepts:: For Information or Comments On This Tutorial, Please Contact R. Frey atEl FaroukNo ratings yet
- Essential guide to human histologyDocument315 pagesEssential guide to human histologyJames Mark Magsipoc OrtegaNo ratings yet
- Lecture notes on human respiratory system physiologyDocument33 pagesLecture notes on human respiratory system physiologyMiles HuiNo ratings yet
- Key Concepts:: For Information or Comments On This Tutorial, Please Contact R. Frey atDocument12 pagesKey Concepts:: For Information or Comments On This Tutorial, Please Contact R. Frey atEl FaroukNo ratings yet
- Hodgkins DiseaseDocument10 pagesHodgkins DiseaseEl FaroukNo ratings yet
- Lecture notes on human respiratory system physiologyDocument33 pagesLecture notes on human respiratory system physiologyMiles HuiNo ratings yet
- Anti Inflamatory Drugs AINSDocument39 pagesAnti Inflamatory Drugs AINSEl FaroukNo ratings yet
- Lect 75control of Tissue Blood FlowDocument23 pagesLect 75control of Tissue Blood FlowEl FaroukNo ratings yet
- Dermatology Questions and AnsDocument147 pagesDermatology Questions and AnsEl FaroukNo ratings yet
- Skin CancerDocument5 pagesSkin CancerEl FaroukNo ratings yet
- Liver CancerDocument3 pagesLiver CancerEl FaroukNo ratings yet
- Survey Whole Circle BearingDocument19 pagesSurvey Whole Circle BearingVin GaragiNo ratings yet
- 3dsmax2013 PU06 Readme0Document6 pages3dsmax2013 PU06 Readme0Divad Zoñum CostaNo ratings yet
- Symmetric GroupDocument13 pagesSymmetric GroupPriyanka PatelNo ratings yet
- Effort Distribution On Waterfall and AgileDocument12 pagesEffort Distribution On Waterfall and Agileanandapramanik100% (2)
- Week 11 - Fundamentals of Distribution SystemsDocument39 pagesWeek 11 - Fundamentals of Distribution SystemsEstika Vriscilla GintingNo ratings yet
- Quantum Garage Door OpenerDocument32 pagesQuantum Garage Door OpenerNguiBDNo ratings yet
- Pritchett Clock Repair Shop Breakeven Analysis ExcelDocument138 pagesPritchett Clock Repair Shop Breakeven Analysis ExcelMohd Yousuf MasoodNo ratings yet
- 1 - Introduction - Derivatives GreeksDocument50 pages1 - Introduction - Derivatives GreeksThomas GallantNo ratings yet
- Definition, Scope and Nature of EconomicsDocument29 pagesDefinition, Scope and Nature of EconomicsShyam Sunder BudhwarNo ratings yet
- LC 72322Document13 pagesLC 72322thecanislupusNo ratings yet
- Answer All The Questions. No Negative Marks For Wrong Answers. Please Do Not Mark Anything On The Question PaperDocument13 pagesAnswer All The Questions. No Negative Marks For Wrong Answers. Please Do Not Mark Anything On The Question PaperMainak DeNo ratings yet
- House of CardsDocument2 pagesHouse of CardsHello misterNo ratings yet
- Discoverer Installation and Integration With EBSDocument25 pagesDiscoverer Installation and Integration With EBSRajendra PrasadNo ratings yet
- Genetic Algorithms TutorialDocument33 pagesGenetic Algorithms Tutorialsuhas199No ratings yet
- Redirection & PipingDocument16 pagesRedirection & PipingPraveen PatelNo ratings yet
- Graph Theory 6Document30 pagesGraph Theory 6Zeeshan AhmedNo ratings yet
- ST RDDocument2 pagesST RDBalteshwar SinghNo ratings yet
- VT2009B Eng 02 953680Document2 pagesVT2009B Eng 02 953680gabrieltracto100% (1)
- AerialSolution - 280 - Brochure - LT - New Design - Final - LRDocument20 pagesAerialSolution - 280 - Brochure - LT - New Design - Final - LRRover DmsNo ratings yet
- Weld-Ing On in Inservice Pipelines - tcm153574190Document7 pagesWeld-Ing On in Inservice Pipelines - tcm153574190Freddy Rondonil SNo ratings yet
- Basic Probability and Reliability Concepts: Roy Billinton Power System Research Group University of Saskatchewan CanadaDocument248 pagesBasic Probability and Reliability Concepts: Roy Billinton Power System Research Group University of Saskatchewan CanadaSimon van BentenNo ratings yet