You might also like
- Pre-Application Enquiry FormDocument4 pagesPre-Application Enquiry FormKevin HarfordNo ratings yet
- Celebrating Eva and Kevin's MarriageDocument13 pagesCelebrating Eva and Kevin's MarriageKevin HarfordNo ratings yet
- Chalkboard Writing TemplateDocument3 pagesChalkboard Writing TemplateKevin HarfordNo ratings yet
- Still Dre Composition PDFDocument2 pagesStill Dre Composition PDFKevin HarfordNo ratings yet
- Lads Who Owe Me TihkDocument2 pagesLads Who Owe Me TihkKevin HarfordNo ratings yet
- The Less I Know The BetterDocument6 pagesThe Less I Know The BetterKevin HarfordNo ratings yet
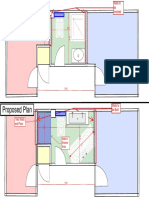
- Bathroom Extension Rev05Document1 pageBathroom Extension Rev05Kevin HarfordNo ratings yet
- Millbank House Plan Drawining PDFDocument1 pageMillbank House Plan Drawining PDFKevin HarfordNo ratings yet
- Take On MSDFGSDGDocument13 pagesTake On MSDFGSDGKevin HarfordNo ratings yet
- Another One - Mac DeMarco - MSCZDocument3 pagesAnother One - Mac DeMarco - MSCZKevin HarfordNo ratings yet
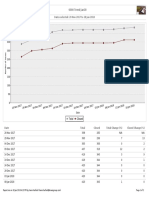
- CLN2-Project Runways 6000 Trend Jan18: Dates Selected: 20 Nov 2017 To 18 Jan 2018Document2 pagesCLN2-Project Runways 6000 Trend Jan18: Dates Selected: 20 Nov 2017 To 18 Jan 2018Kevin HarfordNo ratings yet
- Daily - Weekly.monthly - Responsibilities and ActivitiesDocument1 pageDaily - Weekly.monthly - Responsibilities and ActivitiesKevin HarfordNo ratings yet
- Fallout 4 Main Theme PDFDocument2 pagesFallout 4 Main Theme PDFKevin HarfordNo ratings yet
- Attic ConversionDocument1 pageAttic ConversionKevin HarfordNo ratings yet
- Table Tennis BudgetDocument2 pagesTable Tennis BudgetKevin HarfordNo ratings yet
- Enter the 2014 World Cup Prediction CompetitionDocument17 pagesEnter the 2014 World Cup Prediction CompetitionKevin HarfordNo ratings yet
- Circuit simulation and experimental results comparisonDocument2 pagesCircuit simulation and experimental results comparisonKevin HarfordNo ratings yet
- Circular MotionDocument8 pagesCircular MotionKevin HarfordNo ratings yet
- Dublin Marathon Schedule 2016Document1 pageDublin Marathon Schedule 2016Kevin HarfordNo ratings yet
- Mon Tues Wed Thrs Fri Sat Sun Mon Tues Wed ThrsDocument8 pagesMon Tues Wed Thrs Fri Sat Sun Mon Tues Wed ThrsKevin HarfordNo ratings yet
- Stone/ Ground Works Request Form 32242 CLN Project Runways: Description: (Document1 pageStone/ Ground Works Request Form 32242 CLN Project Runways: Description: (Kevin HarfordNo ratings yet
- REMINDER: Don't Delete or Rename Columns - The Spreadsheet Will Not Import. It Is OK To Delete The Rows Below, Including The Sample DataDocument12 pagesREMINDER: Don't Delete or Rename Columns - The Spreadsheet Will Not Import. It Is OK To Delete The Rows Below, Including The Sample DataKevin HarfordNo ratings yet
- 2800.CLN1-S70155.XX P14MarkedDocument1 page2800.CLN1-S70155.XX P14MarkedKevin HarfordNo ratings yet
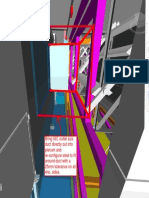
- Bring IAC Outlet Size Duct Directly Out Into Plenum and Re-Configure Steel To Fit Around Duct With A 25mm Tolerance On All 4no. SidesDocument1 pageBring IAC Outlet Size Duct Directly Out Into Plenum and Re-Configure Steel To Fit Around Duct With A 25mm Tolerance On All 4no. SidesKevin HarfordNo ratings yet
- Dublin Marathon Schedule 2016Document1 pageDublin Marathon Schedule 2016Kevin HarfordNo ratings yet
- BaggageDocument4 pagesBaggageKevin HarfordNo ratings yet
- CLN1 6520 MuntersCxDailyUpdate 07 06 17Document2 pagesCLN1 6520 MuntersCxDailyUpdate 07 06 17Kevin HarfordNo ratings yet
- 1000.CLN1 PD TP 0023 - Rev4Document2 pages1000.CLN1 PD TP 0023 - Rev4Kevin HarfordNo ratings yet
- What A Wonderful WorldDocument2 pagesWhat A Wonderful WorldKevin Harford93% (14)
- BaggageDocument4 pagesBaggageKevin HarfordNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Course Outline Legal MedicineDocument6 pagesCourse Outline Legal MedicineMark Howell EsguerraNo ratings yet
- Texting While Driving OutlineDocument4 pagesTexting While Driving OutlineRaelei Noel0% (2)
- United States v. Benancio Cepeda, United States of America v. Ameer Ali Shakoor, 53 F.3d 329, 4th Cir. (1995)Document9 pagesUnited States v. Benancio Cepeda, United States of America v. Ameer Ali Shakoor, 53 F.3d 329, 4th Cir. (1995)Scribd Government DocsNo ratings yet
- DPP Statement On Dams ScandalDocument21 pagesDPP Statement On Dams ScandalThe Star KenyaNo ratings yet
- Television Horror - S - Original - HomeDocument14 pagesTelevision Horror - S - Original - HomeVinicius Azevedo100% (1)
- Cryptocurrency Tax Reporting For FBAR and FATCADocument22 pagesCryptocurrency Tax Reporting For FBAR and FATCAvimal poddarNo ratings yet
- 5 RPC Article 247Document2 pages5 RPC Article 247SexAndSensibilitiesNo ratings yet
- Vanuatu Womens Crisis Research Report Part IDocument83 pagesVanuatu Womens Crisis Research Report Part IZia Ul Haq AliNo ratings yet
- Drug Addiction and Juvenile Delinquency LinkDocument27 pagesDrug Addiction and Juvenile Delinquency LinkNaina MathurNo ratings yet
- Tan Jr Death Penalty Ruling QuestionedDocument2 pagesTan Jr Death Penalty Ruling Questionednojreyam100% (2)
- EconomistsDocument2 pagesEconomistsvarun chandak0% (1)
- ISLaw overviewDocument2 pagesISLaw overviewLU12ROSENo ratings yet
- Mock Board Criminal Law 2Document13 pagesMock Board Criminal Law 2roelalviar100% (9)
- Chapter 5 Computer Fraud: Accounting Information Systems, 13e (Romney/Steinbart)Document15 pagesChapter 5 Computer Fraud: Accounting Information Systems, 13e (Romney/Steinbart)RyzeNo ratings yet
- Application of PenaltiesDocument31 pagesApplication of PenaltiesNivla YacadadNo ratings yet
- Awareness About RapeDocument2 pagesAwareness About RapeAishwarya SundararajNo ratings yet
- Roque vs. People 444 SCRA 98, G.R. No. 138954, November 25, 2004 Qualified TheftDocument6 pagesRoque vs. People 444 SCRA 98, G.R. No. 138954, November 25, 2004 Qualified TheftJerahmeel CuevasNo ratings yet
- PLAINTIFF'S RESPONSE TO DEFENDANTS' TCPA MOTIONS TO DISMISS - Vic Migogna Defamation LawsuitDocument1,188 pagesPLAINTIFF'S RESPONSE TO DEFENDANTS' TCPA MOTIONS TO DISMISS - Vic Migogna Defamation LawsuitAnonymous RtqI2M100% (1)
- RAINCOAT PPT PresentationDocument6 pagesRAINCOAT PPT PresentationFarhan IshrakNo ratings yet
- Waples, Gill, and Fisher - Does CCTV Displace Crime PDFDocument19 pagesWaples, Gill, and Fisher - Does CCTV Displace Crime PDFMiguel Luigi CalayagNo ratings yet
- Constitutional Law 2011Document5 pagesConstitutional Law 2011qanaqNo ratings yet
- Legados Vs de GuzmanDocument2 pagesLegados Vs de GuzmanMaria Cherrylen Castor QuijadaNo ratings yet
- Acid Attack Victims Face Blindness, ScarringDocument2 pagesAcid Attack Victims Face Blindness, ScarringTestNo ratings yet
- United States v. Wright, 4th Cir. (2006)Document3 pagesUnited States v. Wright, 4th Cir. (2006)Scribd Government DocsNo ratings yet
- 2 Internal Audit Roles and ResponsibilitiesDocument26 pages2 Internal Audit Roles and ResponsibilitiesCarlo BaculoNo ratings yet
- Security Verslag GTA Project - 1 Tekst Engels ABdocxDocument27 pagesSecurity Verslag GTA Project - 1 Tekst Engels ABdocxJulius DebatarajaNo ratings yet
- A.K. Subbaiah Vs Karnataka State Bar Council and ... On 19 July, 2002Document6 pagesA.K. Subbaiah Vs Karnataka State Bar Council and ... On 19 July, 2002Pranjul MehtaNo ratings yet
- Script English DramaDocument6 pagesScript English DramaYer CuetoNo ratings yet
- Batas Pambansa Blg. 22: Annotated: Section 1. Checks Without Sufficient Funds. - Any Person Who Makes or DrawsDocument11 pagesBatas Pambansa Blg. 22: Annotated: Section 1. Checks Without Sufficient Funds. - Any Person Who Makes or DrawsJomarco SantosNo ratings yet
- Test Bank Principles of Incident Response and Disaster Recovery 1st Edition WhitmanDocument8 pagesTest Bank Principles of Incident Response and Disaster Recovery 1st Edition Whitmanmarina meshiniNo ratings yet