You might also like
- (Socioanthro) The Beginning of Anthropology and SociologyDocument15 pages(Socioanthro) The Beginning of Anthropology and SociologyAira Alaro100% (1)
- (The Language of Literature) Roger Fowler (Auth.) - The Language of George Orwell-Macmillan Education UK (1995) PDFDocument260 pages(The Language of Literature) Roger Fowler (Auth.) - The Language of George Orwell-Macmillan Education UK (1995) PDFPetr Škaroupka100% (2)
- Head TraumaDocument15 pagesHead TraumaDede Yusuf FNo ratings yet
- Head and Spinal Cord Injury (Ci)Document111 pagesHead and Spinal Cord Injury (Ci)azmerawNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjuryBelle CaharopNo ratings yet
- Introduction to Traumatic Brain InjuryDocument25 pagesIntroduction to Traumatic Brain InjuryRyo JamunNo ratings yet
- Neurosurgey MCQ Collection Part IDocument35 pagesNeurosurgey MCQ Collection Part IMohammed Ali Aldhahir88% (8)
- Head Injury - the silent epidemicDocument52 pagesHead Injury - the silent epidemickarahmanNo ratings yet
- Head InjuryDocument42 pagesHead InjuryMohammad Husni Banisalman100% (3)
- Soal Ujian NeurotraumaDocument22 pagesSoal Ujian NeurotraumaTina HerreraNo ratings yet
- NeuroimagingDocument79 pagesNeuroimagingIdris LubisNo ratings yet
- 39 MCQ's in NeurosurgeryDocument26 pages39 MCQ's in NeurosurgeryAhmed Hamid Ibrahim100% (4)
- DMIT - Midbrain - DMIT SoftwareDocument16 pagesDMIT - Midbrain - DMIT SoftwarevinNo ratings yet
- Clasa 4 Module 5 Lesson 5 ShoppingDocument4 pagesClasa 4 Module 5 Lesson 5 ShoppingviorelcruduNo ratings yet
- PRADEEP'S - Brain TumorDocument32 pagesPRADEEP'S - Brain TumorPRADEEPNo ratings yet
- Head Injuries: Symposium: Combat Casualty CareDocument4 pagesHead Injuries: Symposium: Combat Casualty CareMade GpNo ratings yet
- Head Injury 2: (DR Mohamed A. J. Al Tamimi)Document10 pagesHead Injury 2: (DR Mohamed A. J. Al Tamimi)AmmarNo ratings yet
- A New Classification of Head Injury Based OnDocument7 pagesA New Classification of Head Injury Based OnJejem Marandra EmkamasNo ratings yet
- CraniectomyDocument6 pagesCraniectomyale saenzNo ratings yet
- Imaging of Head Trauma: Part 1: IntroductionDocument28 pagesImaging of Head Trauma: Part 1: Introductiondrnancy1786No ratings yet
- CNS TraumaDocument68 pagesCNS TraumaMonique BorresNo ratings yet
- 7721 (25) NeurotraumaDocument72 pages7721 (25) NeurotraumanewazNo ratings yet
- Cisternostomy: A Timely Intervention in Moderate To Severe Traumatic Brain Injuries: Rationale, Indications, and ProspectsDocument6 pagesCisternostomy: A Timely Intervention in Moderate To Severe Traumatic Brain Injuries: Rationale, Indications, and ProspectsAtul JainNo ratings yet
- J2011.Decompressive Craniectomy Technical NoteDocument6 pagesJ2011.Decompressive Craniectomy Technical NoteKysy CodonNo ratings yet
- Cooper 1992Document7 pagesCooper 1992Edwin Sugondo TaufikNo ratings yet
- Head TraumaDocument5 pagesHead TraumaChynthea ParamithaNo ratings yet
- Epidural Hematoma: Continuing Education ActivityDocument16 pagesEpidural Hematoma: Continuing Education ActivityIka AriandanaNo ratings yet
- Herniasi OtakDocument5 pagesHerniasi OtakrahmaNo ratings yet
- Edh, SDH, & Burr HolesDocument46 pagesEdh, SDH, & Burr HolesRully Riyan DikaNo ratings yet
- Head InjuryDocument30 pagesHead InjuryAngel MakinNo ratings yet
- Emd166 Slide Head InjuryDocument40 pagesEmd166 Slide Head Injuryarikashafa6No ratings yet
- Clinical Characterization of Traumatic Acute Interhemispheric Subdural HematomaDocument7 pagesClinical Characterization of Traumatic Acute Interhemispheric Subdural HematomaDavid Christian HaurissaNo ratings yet
- AADocument4 pagesAARiski novita sari DjamalNo ratings yet
- Causas de Isquemia Na MedulaDocument12 pagesCausas de Isquemia Na MeduladianaNo ratings yet
- Imaging Stroke in MinutesDocument23 pagesImaging Stroke in MinutesAnonymous iea4m0ZRNo ratings yet
- Computed TomographyDocument5 pagesComputed TomographyCrisMartAgullanaNo ratings yet
- Traumatic Intracerebral HemorrhageDocument3 pagesTraumatic Intracerebral HemorrhageTerri Sandi SusyantoNo ratings yet
- Head Injury: From ATLS Chapter 6Document42 pagesHead Injury: From ATLS Chapter 6Elno TatipikalawanNo ratings yet
- Referensi ToxoDocument37 pagesReferensi ToxoAndi IshaqNo ratings yet
- Management of Head InjuriesDocument90 pagesManagement of Head InjuriesrobelNo ratings yet
- Moderate and Severe Traumatic Brain Injury Pathophysiology and ManagementDocument11 pagesModerate and Severe Traumatic Brain Injury Pathophysiology and ManagementRonald Joy DatuNo ratings yet
- Dr. Tayyaba Kiran Lecturer IslamabadDocument45 pagesDr. Tayyaba Kiran Lecturer IslamabadZunairaNo ratings yet
- Skull Base Trauma: Diagnosis and Management: Madjid Samii and Marcos TatagibaDocument10 pagesSkull Base Trauma: Diagnosis and Management: Madjid Samii and Marcos TatagibaYovanka Naryai ManuhutuNo ratings yet
- Clinical Case Presentation: Cerebral Toxoplasmosis in an Immunocompromised PatientDocument12 pagesClinical Case Presentation: Cerebral Toxoplasmosis in an Immunocompromised PatientApriliaNo ratings yet
- Blunt Neck Inj Slides 101217Document45 pagesBlunt Neck Inj Slides 101217taqadasabbasNo ratings yet
- Traumatic Brain Injury: Department of Neurosurgery, The First Affiliated Hospital of Zhengzhou University Xu BinDocument95 pagesTraumatic Brain Injury: Department of Neurosurgery, The First Affiliated Hospital of Zhengzhou University Xu Binapi-19916399No ratings yet
- Polin1997 PDFDocument11 pagesPolin1997 PDFRaul VillacresNo ratings yet
- Cureus 0015 00000037508Document7 pagesCureus 0015 00000037508PeyepeyeNo ratings yet
- 002-Trauma & BurnsDocument35 pages002-Trauma & Burnsmotasem alsharifNo ratings yet
- Head Trauma: Key ConsiderationsDocument1 pageHead Trauma: Key ConsiderationsNawaid KhanNo ratings yet
- Management of Head TraumaDocument15 pagesManagement of Head TraumaBetrice KotanNo ratings yet
- Klumpke Palsy: Merryman J, Varacallo MDocument5 pagesKlumpke Palsy: Merryman J, Varacallo MSuci HandayaniNo ratings yet
- Bacterial Brain Abscess Caused by Klebsiella PneumoniaeDocument9 pagesBacterial Brain Abscess Caused by Klebsiella PneumoniaeNaily Nuzulur RohmahNo ratings yet
- Head Trauma CT Scan Case StudyDocument8 pagesHead Trauma CT Scan Case Studytruevine_ministry100% (1)
- TraumaDocument31 pagesTraumaanwar jabariNo ratings yet
- Aspectos Neurológicos Del Trauma Craneoencefálico IRPDocument10 pagesAspectos Neurológicos Del Trauma Craneoencefálico IRPAndres FierroNo ratings yet
- Neuroimaging of Stroke (Early Signs On CT and MRI)Document48 pagesNeuroimaging of Stroke (Early Signs On CT and MRI)erickoteNo ratings yet
- Depressed Fracture NSMC - AbstractDocument14 pagesDepressed Fracture NSMC - AbstractGlen Sandy SaapangNo ratings yet
- Chest Wall, Pneumothorax, and Hemothorax: Brain DeathDocument5 pagesChest Wall, Pneumothorax, and Hemothorax: Brain DeathMelly SyafridaNo ratings yet
- Traumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuDocument38 pagesTraumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuAnna DianaNo ratings yet
- ER CASES RDocument32 pagesER CASES RHarris ShaikhNo ratings yet
- Coles TBIDocument12 pagesColes TBIhalamadrid77No ratings yet
- Journal of International Medical Research 2009 Zhu 983 95Document13 pagesJournal of International Medical Research 2009 Zhu 983 95Annisa ChastallaNo ratings yet
- Trauma Kepala Dan MielumDocument168 pagesTrauma Kepala Dan Mielumnatalia nancy0% (1)
- Complications of Percutaneous Coronary Intervention: The Survival HandbookFrom EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNo ratings yet
- Clinical Pathway Limphadenopaty ColiDocument6 pagesClinical Pathway Limphadenopaty ColiTina HerreraNo ratings yet
- Clinical Pathway for Inguinal Hernia RepairDocument6 pagesClinical Pathway for Inguinal Hernia RepairTina HerreraNo ratings yet
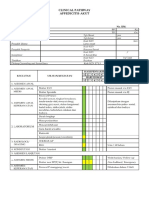
- CP AppendectomyDocument6 pagesCP AppendectomyTina HerreraNo ratings yet
- 167 FullDocument5 pages167 FullTina HerreraNo ratings yet
- Jurnal PoneDocument21 pagesJurnal PoneTina HerreraNo ratings yet
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocument9 pagesComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraNo ratings yet
- Aaam Face Thread c5 2019 FlyerDocument1 pageAaam Face Thread c5 2019 FlyerTina HerreraNo ratings yet
- Pie 2018Document5 pagesPie 2018Tina HerreraNo ratings yet
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocument9 pagesComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraNo ratings yet
- Clinical Pathway Apendisitis AcutaDocument7 pagesClinical Pathway Apendisitis AcutaTina HerreraNo ratings yet
- Tumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastDocument26 pagesTumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastTina HerreraNo ratings yet
- Aaam Face Thread c5 2019 FlyerDocument1 pageAaam Face Thread c5 2019 FlyerTina HerreraNo ratings yet
- Controversy in Head Injury, Abdul Hafid PDFDocument31 pagesControversy in Head Injury, Abdul Hafid PDFTina HerreraNo ratings yet
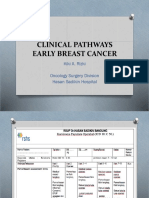
- CP Early Breast CancerDocument8 pagesCP Early Breast CancerTina HerreraNo ratings yet
- Controversy in Head Injury, Abdul Hafid PDFDocument31 pagesControversy in Head Injury, Abdul Hafid PDFTina HerreraNo ratings yet
- Pharmacotherapy of Traumatic Brain Injury (2015)Document6 pagesPharmacotherapy of Traumatic Brain Injury (2015)Tina HerreraNo ratings yet
- Guia de Bologna-2013Document14 pagesGuia de Bologna-2013andreigustvNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Thoracic Lumbar, Eko AgusDocument32 pagesThoracic Lumbar, Eko AgusTina HerreraNo ratings yet
- Biomolecular and Immunological, Sofia MDocument64 pagesBiomolecular and Immunological, Sofia MTina HerreraNo ratings yet
- Pre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Document7 pagesPre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Tina HerreraNo ratings yet
- Outcome of Surgically Treated Traumatic Extradural Hematoma (2016)Document9 pagesOutcome of Surgically Treated Traumatic Extradural Hematoma (2016)Tina HerreraNo ratings yet
- National Guideline, Peter LDocument51 pagesNational Guideline, Peter LTina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Biomelecular Aspect, Irawan YusufDocument23 pagesBiomelecular Aspect, Irawan YusufTina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Jurnal NCDocument12 pagesJurnal NCTina HerreraNo ratings yet
- Calla LessonDocument3 pagesCalla Lessonapi-283263408No ratings yet
- Science TeachersDocument16 pagesScience TeachersNashwaNo ratings yet
- Song Lyrics Analysis LessonDocument3 pagesSong Lyrics Analysis Lessonsarah gaia ruoccoNo ratings yet
- Linguistic Varieties and Multilingual NationsDocument21 pagesLinguistic Varieties and Multilingual NationsDesya Kurnia SaputriNo ratings yet
- Uni 1 gw5 - TestDocument3 pagesUni 1 gw5 - TestDebora AlmeidaNo ratings yet
- CPM 1 - Fundamental Elements of Project ManagementDocument22 pagesCPM 1 - Fundamental Elements of Project ManagementlukeNo ratings yet
- Happinessmeaning Course Description-2Document4 pagesHappinessmeaning Course Description-2api-242468651No ratings yet
- Bangladesh Madrasah Education Board Name Correction DecisionsDocument2 pagesBangladesh Madrasah Education Board Name Correction DecisionsImamNo ratings yet
- 10 Ways To Say Hello & GoodbyeDocument151 pages10 Ways To Say Hello & GoodbyeDavid Kyaw100% (1)
- ESL 064 ADV 1 Reading Spring 2 2023 VedoveliDocument7 pagesESL 064 ADV 1 Reading Spring 2 2023 VedoveliANTHONY PINONo ratings yet
- Understanding Student-Centered Learning and Philosophies of Teaching PracticesDocument7 pagesUnderstanding Student-Centered Learning and Philosophies of Teaching PracticesFikri Arvitesar IINo ratings yet
- DepEd NCR calls for 2022 Basic Education Research Fund proposalsDocument40 pagesDepEd NCR calls for 2022 Basic Education Research Fund proposalsMaestra Ligaya Maria YojNo ratings yet
- Especulation As Mode of ProductionDocument266 pagesEspeculation As Mode of ProductionAndrea GarcésNo ratings yet
- Implementation of Anti-Smoking Ordinance ThesisDocument11 pagesImplementation of Anti-Smoking Ordinance ThesisBOLINANo ratings yet
- GowthamDocument2 pagesGowthammaniNo ratings yet
- Interview QuestionsDocument5 pagesInterview QuestionsKailash KumarNo ratings yet
- UDP I Course Syllabus 2023Document3 pagesUDP I Course Syllabus 2023Addiswork AnleyNo ratings yet
- Guinto, Critique PaperDocument4 pagesGuinto, Critique PaperReanne GuintoNo ratings yet
- Paris City of LightDocument3 pagesParis City of LightJohn Felix SitumorangNo ratings yet
- Project FailureDocument2 pagesProject FailureankiroteNo ratings yet
- Standardization of Ficus Religiosa Seed ExtractDocument5 pagesStandardization of Ficus Religiosa Seed ExtractAnshu Kumar SinhaNo ratings yet
- Japanese Industrialization and Economic GrowthDocument5 pagesJapanese Industrialization and Economic GrowthsmrithiNo ratings yet
- Syllabus - Middle School WritingDocument11 pagesSyllabus - Middle School Writingmrspercuoco100% (2)
- Department of FoodDocument2 pagesDepartment of FoodBhushan DevraniNo ratings yet
- Lesson Plan 3 Fairy Tale Narration - Clinical 429Document6 pagesLesson Plan 3 Fairy Tale Narration - Clinical 429api-176688637No ratings yet
- Manual of Architectural PracticeDocument95 pagesManual of Architectural PracticeGabby xxxNo ratings yet