You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Substance Abuse Counseling Complete 5th EditionDocument379 pagesSubstance Abuse Counseling Complete 5th Editionnintendoagekid86% (59)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Nursing School Necessities Cheat SheetDocument3 pagesNursing School Necessities Cheat SheetRevNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- School District of Philadelphia's Immigrant & Refugee ToolkitDocument58 pagesSchool District of Philadelphia's Immigrant & Refugee ToolkitKristina KoppeserNo ratings yet
- Baseline Risk Assessment and Risk Matrix (An Example)Document8 pagesBaseline Risk Assessment and Risk Matrix (An Example)Victor75% (4)
- Template Clerking PsychiatryDocument2 pagesTemplate Clerking Psychiatrymunii28No ratings yet
- Hyaluronic Acid Injections For Treatment Of.2Document7 pagesHyaluronic Acid Injections For Treatment Of.2CitraNo ratings yet
- Asset Integrity Know HowDocument6 pagesAsset Integrity Know HowFatemeh MehrbakhshNo ratings yet
- Dementia Rating ScaleDocument2 pagesDementia Rating ScaleIqbal BaryarNo ratings yet
- TOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaDocument24 pagesTOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaRedmond P. Burke MD100% (1)
- Morning Report: Abdominal TraumaDocument10 pagesMorning Report: Abdominal TraumaJAQUELINENo ratings yet
- Morning Report Wati Dan EvaDocument20 pagesMorning Report Wati Dan EvaJAQUELINENo ratings yet
- Morning Report: Abdominal TraumaDocument10 pagesMorning Report: Abdominal TraumaJAQUELINENo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaJAQUELINENo ratings yet
- International Journal of Health Sciences and ResearchDocument10 pagesInternational Journal of Health Sciences and ResearchJAQUELINENo ratings yet
- Pi Is 0952818016307279Document6 pagesPi Is 0952818016307279doktersandraNo ratings yet
- Neurodermatitis Referat: Lichen Simplex ChronicDocument12 pagesNeurodermatitis Referat: Lichen Simplex ChronicJAQUELINENo ratings yet
- 3348 14080 1 PBDocument3 pages3348 14080 1 PBFrishia DidaNo ratings yet
- Jurnal ICU 1Document7 pagesJurnal ICU 1JAQUELINENo ratings yet
- Quar Esma 2014Document2 pagesQuar Esma 2014JAQUELINENo ratings yet
- Jurnal Anastesi 2Document6 pagesJurnal Anastesi 2JAQUELINENo ratings yet
- Jurnal Anastesi 3Document8 pagesJurnal Anastesi 3JAQUELINENo ratings yet
- Morning Report: Abdominal TraumaDocument10 pagesMorning Report: Abdominal TraumaJAQUELINENo ratings yet
- Edit Prak CVDDocument35 pagesEdit Prak CVDAliatunnisa SidangNo ratings yet
- Praktikum Cardiovaskular DiseaseDocument38 pagesPraktikum Cardiovaskular DiseaseJAQUELINENo ratings yet
- Jurnal 1Document10 pagesJurnal 1JAQUELINENo ratings yet
- Bjsports 2016 096142Document9 pagesBjsports 2016 096142JAQUELINENo ratings yet
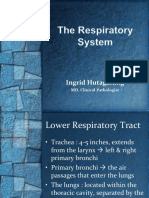
- Pengantar Sistem RespirasiDocument23 pagesPengantar Sistem RespirasiJAQUELINENo ratings yet
- Jurnal 7Document6 pagesJurnal 7JAQUELINENo ratings yet
- Jurnal 5Document7 pagesJurnal 5JAQUELINENo ratings yet
- 2016 Article 1149Document12 pages2016 Article 1149JAQUELINENo ratings yet
- Arthritis R UKDocument40 pagesArthritis R UKAbdulziz Al-jedaieNo ratings yet
- P 49Document8 pagesP 49JAQUELINENo ratings yet
- Viscosupplementation For Osteoarthritis of The KneeDocument14 pagesViscosupplementation For Osteoarthritis of The KneeJAQUELINENo ratings yet
- Bjsports 2016 096142Document9 pagesBjsports 2016 096142JAQUELINENo ratings yet
- Viscosupplementation For Osteoarthritis of The KneeDocument14 pagesViscosupplementation For Osteoarthritis of The KneeJAQUELINENo ratings yet
- J Neurol Neurosurg Psychiatry 2001 Muir I12 6Document6 pagesJ Neurol Neurosurg Psychiatry 2001 Muir I12 6JAQUELINENo ratings yet
- Jaqueline Mawarni Effendy (2012-83-044)Document15 pagesJaqueline Mawarni Effendy (2012-83-044)JAQUELINENo ratings yet
- ResearchSTEM 12Document77 pagesResearchSTEM 12JhanelNo ratings yet
- Jakarta Cardiovascular Care Unit Network System OverviewDocument52 pagesJakarta Cardiovascular Care Unit Network System OverviewekaNo ratings yet
- SPS321 Sports Safety and Emergency Care Mohd Fadzil B. Hj. Kamarudin Sr113 Uitm/InstedtDocument9 pagesSPS321 Sports Safety and Emergency Care Mohd Fadzil B. Hj. Kamarudin Sr113 Uitm/InstedtMozil Fadzil KamarudinNo ratings yet
- Manajemen Pemeliharaan Puyuh Periode Layer Di CV Agri Bird Karanganyar Jawa TengahDocument54 pagesManajemen Pemeliharaan Puyuh Periode Layer Di CV Agri Bird Karanganyar Jawa TengahRyah NurNo ratings yet
- Antiparkinsonian Drugs Pathophysiology and TreatmentDocument5 pagesAntiparkinsonian Drugs Pathophysiology and Treatmentkv 14No ratings yet
- Progress Test 04Document6 pagesProgress Test 04Lemmy the GamerNo ratings yet
- Chronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISDocument4 pagesChronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISJuanEstebanOspinaNo ratings yet
- Declaration of Erin EllisDocument4 pagesDeclaration of Erin EllisElizabeth Nolan BrownNo ratings yet
- Essay On Current Poverty State of India After COVID-19: KeywordsDocument10 pagesEssay On Current Poverty State of India After COVID-19: KeywordsMALLI ROYALNo ratings yet
- Nursing Audit ScheduleDocument2 pagesNursing Audit ScheduleArvinjohn Gacutan0% (1)
- From MaureenDocument1 pageFrom MaureenWKYC.comNo ratings yet
- Drug in PregnancyDocument5 pagesDrug in PregnancyjokosudibyoNo ratings yet
- Overcoming The Pilot Shortage PDFDocument16 pagesOvercoming The Pilot Shortage PDFTim ChongNo ratings yet
- Introduction To Psychology BrochureDocument2 pagesIntroduction To Psychology BrochureErika JimenezNo ratings yet
- Kerry Washington. Family Secret.Document3 pagesKerry Washington. Family Secret.yulya.shevchenko110No ratings yet
- Corn SpecDocument4 pagesCorn SpecJohanna MullerNo ratings yet
- 2001SimulationCompet PDFDocument15 pages2001SimulationCompet PDFdaselknamNo ratings yet
- PE 11 Cardio Endurance Workout ReflectionsDocument2 pagesPE 11 Cardio Endurance Workout ReflectionsFranky MendozaNo ratings yet
- BSN 3G GRP 4 Research TitlesDocument6 pagesBSN 3G GRP 4 Research TitlesUjean Santos SagaralNo ratings yet
- Semi Solids PDFDocument3 pagesSemi Solids PDFAsif Hasan NiloyNo ratings yet
- HRFuture Sept 2020 MJLKJDocument59 pagesHRFuture Sept 2020 MJLKJGlecy KimNo ratings yet
- Drug Study Kalium DuruleDocument2 pagesDrug Study Kalium DuruleGrant Kenneth Dumo AmigableNo ratings yet