You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Freddie My LoveDocument8 pagesFreddie My LoveRacheal YoungNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Personal Development GoalsDocument10 pagesPersonal Development GoalsGeorgia Stewart100% (1)
- Sustainable Building MaterialsDocument8 pagesSustainable Building MaterialsRaghavi SathyaNo ratings yet
- 13 Principles of Business LawDocument471 pages13 Principles of Business Lawyssuf100% (3)
- Norton Leslie - Léonide Massine and The 20th Century BalletDocument381 pagesNorton Leslie - Léonide Massine and The 20th Century BalletManuel CoitoNo ratings yet
- SUMMARYDocument44 pagesSUMMARYGenelle Mae MadrigalNo ratings yet
- A Manual of Cost Cuts For Strong Acceptable HousingDocument74 pagesA Manual of Cost Cuts For Strong Acceptable HousinggeaswaranNo ratings yet
- Mycobacterium TuberculosisDocument54 pagesMycobacterium TuberculosisDaniel WaweruNo ratings yet
- CSR Project Report On NGODocument41 pagesCSR Project Report On NGOabhi ambre100% (3)
- Bank Secrecy Law ExceptionsDocument5 pagesBank Secrecy Law Exceptionsjb_uy100% (1)
- 14 Patterns of Biophilic Design Terrapin 2014e PDFDocument64 pages14 Patterns of Biophilic Design Terrapin 2014e PDFRaghavi SathyaNo ratings yet
- Katherine Museum New Building Concept DesignDocument22 pagesKatherine Museum New Building Concept DesignDivya Nair50% (2)
- Facepot AmigurumiDocument10 pagesFacepot AmigurumiAna Laura Marçal Monsores100% (2)
- London - Serpentine Pavilion 2016 by BIG Bjarke Ingels GroupDocument10 pagesLondon - Serpentine Pavilion 2016 by BIG Bjarke Ingels GroupRaghavi SathyaNo ratings yet
- Restoring With A Touch of Basic Design PDFDocument1 pageRestoring With A Touch of Basic Design PDFRaghavi SathyaNo ratings yet
- Dal Char Housing IssuesDocument1 pageDal Char Housing IssuesRaghavi SathyaNo ratings yet
- Fire Accidents and Safety MeasuresDocument5 pagesFire Accidents and Safety MeasuresRaghavi SathyaNo ratings yet
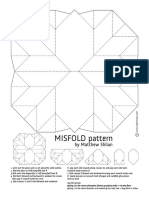
- MI Sfold Pat T Er N: by Mat T Hew SHL I AnDocument1 pageMI Sfold Pat T Er N: by Mat T Hew SHL I AnRaghavi SathyaNo ratings yet
- 0321969073Document18 pages0321969073Raghavi SathyaNo ratings yet
- 15 Million Elderly Indians Live All Alone - Census - Times of IndiaDocument3 pages15 Million Elderly Indians Live All Alone - Census - Times of IndiaRaghavi SathyaNo ratings yet
- ElderlyinIndia 2016 PDFDocument104 pagesElderlyinIndia 2016 PDFRaghavi SathyaNo ratings yet
- Book On Architectural CompetitionsDocument98 pagesBook On Architectural CompetitionsRaghavi SathyaNo ratings yet
- Building Materials I: Soil Fundamentals and ClassificationDocument24 pagesBuilding Materials I: Soil Fundamentals and ClassificationRaghavi SathyaNo ratings yet
- Laurie Baker-Mud Hindi EnglishDocument47 pagesLaurie Baker-Mud Hindi EnglishkhanNo ratings yet
- Soil Stab-Use Of-New - PPT DR MSA Edusat - PPT Rev 1Document75 pagesSoil Stab-Use Of-New - PPT DR MSA Edusat - PPT Rev 1Vinod KumarNo ratings yet
- Area Per PersonDocument2 pagesArea Per PersonRaghavi SathyaNo ratings yet
- A Study On Influences of Lighting On Resource Usage in An Institution LibraryDocument4 pagesA Study On Influences of Lighting On Resource Usage in An Institution LibraryRaghavi SathyaNo ratings yet
- Research Methodology-Dr - Faiz - Part IDocument33 pagesResearch Methodology-Dr - Faiz - Part IRaghavi SathyaNo ratings yet
- Architectural Case Study 1, Nit TrichyDocument6 pagesArchitectural Case Study 1, Nit TrichyRaghavi SathyaNo ratings yet
- Area Per PersonDocument2 pagesArea Per PersonRaghavi SathyaNo ratings yet
- Zero Carbon New Non-Domestic Buildings Consultation ReportDocument19 pagesZero Carbon New Non-Domestic Buildings Consultation ReportChoo Wei Ee DansonNo ratings yet
- Real Vs VirtualDocument8 pagesReal Vs VirtualRaghavi SathyaNo ratings yet
- Phần 30 câu trắc nghiệm tiếng AnhDocument5 pagesPhần 30 câu trắc nghiệm tiếng AnhVinh HàNo ratings yet
- #4 Lacurom vs. Tienzo 535 SCRA 253, Oct 9 2007 FactsDocument12 pages#4 Lacurom vs. Tienzo 535 SCRA 253, Oct 9 2007 FactsDana Denisse RicaplazaNo ratings yet
- SBPD Discipline MatrixDocument8 pagesSBPD Discipline MatrixLeah MoreauNo ratings yet
- ArtmuseumstoexploreonlineDocument1 pageArtmuseumstoexploreonlineapi-275753499No ratings yet
- Compare Quickbooks Plans: Buy Now & Save Up To 70%Document1 pageCompare Quickbooks Plans: Buy Now & Save Up To 70%Agustus GuyNo ratings yet
- Cra Law Virtua 1aw Lib RaryDocument29 pagesCra Law Virtua 1aw Lib RaryGabbie DionisioNo ratings yet
- Rights and Welfare for Philippine Native Dogs (AspinDocument15 pagesRights and Welfare for Philippine Native Dogs (AspinJenilyn ZapantaNo ratings yet
- Adverbs, Adjectives, Genitive TeorieDocument4 pagesAdverbs, Adjectives, Genitive TeorieMihaela ParvuNo ratings yet
- Exam Call Letter Clerk RecruitmentDocument2 pagesExam Call Letter Clerk RecruitmentBala SubramanianNo ratings yet
- Mark Carney Oxford ThesisDocument6 pagesMark Carney Oxford Thesisgj9zvt51100% (1)
- UK Health Forum Interaction 18Document150 pagesUK Health Forum Interaction 18paralelepipicoipiNo ratings yet
- Ten Anglican ChantsDocument10 pagesTen Anglican ChantsAndrew WrangellNo ratings yet
- Endorsement Letter From The Head of InstitutionDocument2 pagesEndorsement Letter From The Head of InstitutionkavinNo ratings yet
- Ningam Siro NR Parmar OverruledDocument32 pagesNingam Siro NR Parmar OverruledSardaar Harpreet Singh HoraNo ratings yet
- Pernille Gerstenberg KirkebyDocument17 pagesPernille Gerstenberg KirkebymanufutureNo ratings yet
- Scenario - River Spray Company Was Organized To Gro...Document5 pagesScenario - River Spray Company Was Organized To Gro...Ameer Hamza0% (1)
- QSCL035284B Air Quote For Expeditors Chile Transportes Internacionales Limitada - OSL - SCL - P0640220Document2 pagesQSCL035284B Air Quote For Expeditors Chile Transportes Internacionales Limitada - OSL - SCL - P0640220MINEC SpANo ratings yet
- Module in Mapeh 7: Directions: Do You Have A Diary? Where You Able To Make One? Write in Your DiaryDocument4 pagesModule in Mapeh 7: Directions: Do You Have A Diary? Where You Able To Make One? Write in Your DiaryChristian Gonzales LaronNo ratings yet
- 6 - Overview of NEC - 2023Document112 pages6 - Overview of NEC - 2023Ka Yu YeungNo ratings yet
- Final Design E-Portfolio Main Criteria A-B-CDocument22 pagesFinal Design E-Portfolio Main Criteria A-B-Capi-540488192No ratings yet
- Objectives of Community Based RehabilitationDocument2 pagesObjectives of Community Based Rehabilitationzen_haf23No ratings yet
- Odisha PWD Registration in CDMSDocument2 pagesOdisha PWD Registration in CDMSSabyasachi Naik (Zico)No ratings yet