Professional Documents
Culture Documents
DR Bowo
Uploaded by
AnthonyJohanOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
DR Bowo
Uploaded by
AnthonyJohanCopyright:
Available Formats
Genitourinar y Imaging Original Research
use only; all rights reserved
Diagnostic Yield of CT Urography
in the Evaluation of Young Adults
With Hematuria
1 OBJECTIVE. CT urography is increasingly used as the initial imaging test in patients with
R. Peter Lokken
Downloaded from www.ajronline.org by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal
Cheryl A. Sadow hematuria. The aim of our study was to determine the yield of CT urography in young adults with
Stuart G. Silverman hematuria to see whether single phase unenhanced CT would have been sufficient.
MATERIALS AND METHODS. We reviewed medical records of consecutive patients
undergoing CT urography between March 2000 and July 2009 at our tertiary medical cen-ter.
Of 5400 CT urograms performed, 375 (6.9%) in 359 patients aged 40 years or younger with
hematuria were included in the study. Urographic findings were tabulated according to their
clinical significance. CT images were reviewed to see whether contrast-enhanced im-ages
were necessary for diagnosis.
RESULTS. A clinically significant source was found in 83 of 375 examinations (22.1%),
including 42 of 142 (29.6%) for gross hematuria, 29 of 181 (16.0%) for microscopic
hematu-ria, and 12 of 52 (23.1%) for hematuria of unspecified subtype. The most common
clinically significant findings were renal or ureteral calculi (n = 73 [75.3%]); four
malignancies were also detected. Ninety-two (94.8%) of 97 clinically significant findings
were evident on unen-hanced images. All significant findings that required contrast-
enhanced images for diagnosis occurred in patients with predisposing medical conditions.
CONCLUSION. A clinically significant source of hematuria was detected in 22.1% of
CT urograms of young adults. However, an unenhanced CT alone may be sufficient in pa-
tients without additional predisposing medical conditions, thereby reducing radiation dose in
this radiosensitive population.
ematuria is a common urologic H finding in
young adults, reported in 0.338.7% of adults in
adults with microscopic hematuria [3]. The
increasing use of CT urography as the initial
popula-tion-based studies [13]. Gross imaging test raises additional concerns
hematuria has a relatively high predictive about radiation exposure to this
value for malignancy and therefore warrants radiosensitive pop-ulation [1517].
a thorough urologic evaluation [4, 5]. We therefore examined the diagnostic
Asymptomatic microscopic hematuria rarely yield of CT urography in young adults eval-
Keywords: CT urography, gross hematuria, hematuria, signals a life-threatening condition and is uated for hematuria at our institution to de-
microscopic hematuria, upper urinary tract most often a benign incidental finding [68]. termine whether the increased radiation dose
The appropriate strategy for imaging young compared with excretory urography or a sin-
DOI:10.2214/AJR.11.7296
adults with microscopic hematuria has there- gle phase unenhanced CT is indicated.
Received May 30, 2011; accepted after fore been controversial.
revision July 21, 2011. Current guidelines from the American Materials and Methods
1 Urologic Association and American College of This retrospective single-center cohort study
All authors: Department of Radiology, Division
Radiology recommend upper urinary tract was HIPAA-compliant. Institutional review board
of Abdominal Imaging and Intervention,
Brigham and Womens Hospital, 75 Francis St, imaging of adults with excretory urography or approval was obtained before initiation of the
Boston, MA 02115. Address correspondence to CT urography [9, 10]. However, many studies study, with waiver of informed consent for review
R. P. Lokken (rlokken@partners.org). have found few clinically signifi-cant upper of medical records.
urinary tract findings in patients aged 40 years We retrospectively reviewed medical records of
AJR 2012; 198:609615
and younger [1114], leading some to question all patients who underwent CT urography at our
0361803X/12/1983609 the need to image all young tertiary academic medical center between March
2000 and July 2009 to identify examinations
American Roentgen Ray Society
AJR:198, March 2012 609
Lokken et al.
TABLE 1: Sources of Hematuria Identified in 375 CT Urograms Performed in Patients Aged 40 Years or Younger
No. of Positive Findings, by Type of Hematuria
Findings Evident on Unenhanced
Category, Diagnosis Gross Microscopic Unspecified Images, No./Total (%)
Life threatening
Lymphoma 0 0 1 0/1 (0.0)
Metastatic testicular cancer 1 0 0 1/1 (100.0)
by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal use only; all rights reserved
Metastatic Ewing sarcoma 1 0 0 1/1 (100.0)
Renal mass 1 0 0 1/1 (100.0)
Renal laceration 1 0 0 1/1 (100.0)
Total 4 0 1 4/5 (80.0)
Significant, requiring treatment
Renal calculus 29 18 10 57/57 (100.0)
Ureteral calculus 9 5 2 16/16 (100.0)
Ureteropelvic junction obstruction 2 1 0 3/3 (100.0)
Bacterial cystitis 1 0 0 0/1 (0.0)
Colovesical fistula 1 0 0 1/1 (100.0)
Medullary nephrocalcinosis 0 2 0 2/2 (100.0)
Hemorrhagic cystitis 1 0 0 1/1 (100.0)
Pyelonephritis 0 1 0 0/1 (0.0)
Ureteral transection 0 1 0 1/1 (100.0)
Total 43 28 12 81/83 (97.6)
Significant, requiring observation
Atrophic kidney 1 3 0 4/4 (100.0)
Neurogenic bladder 2 0 0 1/2 (50.0)
Benign prostatic hyperplasia 0 0 1 1/1 (100.0)
Interstitial cystitis 0 1 0 1/1 (100.0)
Papillary necrosis 0 1 0 0/1 (0.0)
Total 3 5 1 7/9 (77.8)
Insignificant
Renal cyst (Bosniak category I or II) 23 24 7 37/54 (68.5)
Duplicated collecting system 4 1 1 3/6 (50.0)
Renal parenchymal scarring 3 3 0 4/6 (66.7)
Calyceal diverticulum 0 1 1 1/2 (50.0)
Total 30 29 9 45/68 (66.2)
performed on patients 40 years of age or younger for We reviewed imaging reports of included studies, who was blinded to the imaging report and to
Downloaded from www.ajronline.org
the primary indication of hematuria. On the basis of rendered by 14 abdominal radiologists with 125 whether the study contained a true- or false-
information available in the medical record, years of experience interpreting CT examinations, to positive finding. The reviewer first attempted to
hematuria was classified as microscopic, gross, or evaluate whether a potential source of hematuria was identify sources of hematuria by examining axial
unspecified subtype. A total of 5400 CT urographic detected. Follow-up examinations and clinical data in unenhanced phase images alone. If the reviewer
examinations were performed during this period, the medical record were reviewed to determine identified a potential abnormality on unenhanced
including 829 examinations (15.4%) in patients 40 whether these findings were true- or false-positives. images but requested contrast-enhanced phases
years or younger. Of these, 375 examinations in 359 True-positive findings were tabulated according to for further characterization, the finding was also
patients were performed for the primary indication of their clinical significance as specified by the tabulated as visible on unenhanced images. If no
hematuria, including gross (n = 142), microscopic (n American Urologic Association Best Practice Policy finding was detected, the reviewer then evaluated
= 181), and hematuria of unspecified subtype (n = Guidelines [8]. the contrast-enhanced images. If findings were
52). The patient population included 150 male and Imaging studies with true- and false-positive detected only on contrast-enhanced images, they
209 female patients (age range, 16 40 years; mean findings were reviewed by a radiologist with 9 were tabulated as requiring contrast-enhanced
SD, 32.7 6.0 years). years of experience interpreting CT urography images for detection. If the reviewer did not
610 AJR:198, March 2012
CT Urography to Evaluate Hematuria in Young Adults
0.8751.25 pitch, 120 kVp, and 155280 mA) and a
synchronous nephrographic and excretory phase scan
(0.61.0 mm collimation, 0.651.00 pitch, 120 kVp,
and 160180 mA) of the abdomen and pelvis that
followed an initial dose of contrast medium, a 6-
minute delay, a second dose of contrast medium, and
imaging acquisition at 100 seconds after the second
dose of contrast [19]. During the period when the
115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal use only; all rights reserved
split-bolus scans were performed, protocols varied
slightly using different combinations of contrast
medium dosing with either 150 mL total of
iopromide 300 or 120 mL of iopromide 370.
Results
A B
We identified 165 findings associated with
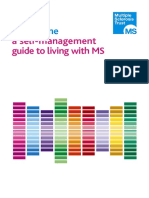
Fig. 140-year-old man who had episode of painless gross hematuria. hematuria in 132 (35.2%) of the 375 CT uro-
A, Axial nephrographic phase image of CT urogram shows heterogeneously enhancing 6.4-cm right
upper pole renal mass (arrow) suspicious for renal cell carcinoma.
grams; of these findings, 97 (58.8%) findings
B, Renal mass was evident on unenhanced image. Patient was lost to follow-up before in 83 examinations (22.1%) were clinically
pathologic specimen was obtained. significant (Table 1). The yield of CT urog-
raphy for clinically significant findings was
29.6% (42/142 CT urograms) for patients with
gross hematuria, 16.0% (29/181) for mi-
croscopic hematuria, and 23.1% (12/52) for
hematuria of unspecified subtype.
Four of five life-threatening findings were
tumors; the other was a renal laceration in a
patient who had sustained a biking accident.
Four of the life-threatening findings, including
metastatic testicular cancer, metastatic Ewing
sarcoma, a probable renal cell carcinoma (Fig.
1), and the renal laceration, were evident on
unenhanced images. A hypoenhancing renal
A B mass suspicious for tumor involvement in a
patient with non-Hodgkin lymphoma and new
Fig. 223-year-old woman with non -Hodgkin lymphoma who developed hematuria and
abdominal pain while undergoing chemotherapy. CT urogram was performed, and oral contrast onset of hematuria required contrast-enhanced
agent was administered for concurrent cancer staging. images for detection (Fig. 2).
A, Axial nephrographic phase image shows hypoenhancing 3.4-cm right renal mass (arrow) There were 83 findings in 72 studies that
suspicious for tumor.
B, Renal mass was not detected on unenhanced image. were significant and required treatment; 81
(97.6%) of these findings were detectable on
unenhanced images. The majority of these
detect the finding on any images, the study was Before January 2004, patients were scanned by findings were renal (n = 49 [59.0%]) or ure-
then shown to an adjudicator with 25 years of using a three-scan CT protocol, including an teral (n = 15 [18.1%]) calculi, all of which
Downloaded from www.ajronline.org by
experience interpreting CT examinations, who unenhanced scan (0.62.5 mm collimation, 0.875 were evident on unenhanced images. One
determined whether the finding was present on 1.25 pitch, 120 kVp, and 155280 mA) of the ureteral calculus was detected by the blind-
unenhanced or contrast-enhanced images. abdomen and pelvis, a nephrographic phase scan of ed reviewer on unenhanced images as either
CT urography was performed with 4-, 16-, 64-, the kidneys (0.62.5 mm collimation, 0.8751.25 a ureteral calculus or phlebolith; the diag-
or 128-MDCT scanners (Somatom Volume Zoom, pitch, 120 kVp, and 155280 mA) 100 seconds after nosis of ureteral calculus was confirmed on
Somatom Sensation 16, Somatom Sensation 64, IV contrast administration of 100 mL of iopromide contrast-enhanced images. One 1-mm re-nal
and Definition AS 128, all from Siemens (Ultravist 300, Berlex Laboratories) at 3 mL/s, and an calculus and one 2-mm ureteral calculus
Healthcare; and Aquilion 64 and Aquilion 320, excretory phase scan of the abdomen and pelvis (0.6 were not detected on either unenhanced or
both from Toshiba). Patients were asked to void 1.0 mm collimation, 0.651.00 pitch, 120 kVp, and contrast-enhanced images by the blinded re-
immediately before the examination and to drink 160180 mA) 15 minutes after contrast injection viewer but were detected by the adjudicator
900 mL of water. Examinations were [18]. Excretory phase scans were reconstructed at on unenhanced images.
supplemented with either 250 mL of IV saline 3-to 5-mm-thick sections in the axial plane and 3- Two findings that were significant and re-
after instillation of 10 mg of IV furosemide mm-thick sections in the coronal plane. quired treatment were detected on contrast-
(Lasix, Abbott Laboratories) administered 23 Beginning January 2004, patients were scanned by enhanced images only. One was bacterial
minutes before contrast medium, or both [18]. using a two-scan split-bolus protocol, including an cystitis in a patient with recurrent microscop-ic
Patients were scanned in the supine position. unenhanced scan (0.62.5 mm collimation, hematuria and urinary urgency. Concur-
AJR:198, March 2012 611
Lokken et al.
www.ajronline.org by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal use only; all rights reserved
A B C
Fig. 340-year-old woman with multiple sclerosis, recurrent urinary tract infections, and neurogenic bladder evaluated for microscopic hematuria.
A and B, Coronal (A) and axial (B) images from excretory phase CT urogram show clubbed calyces (arrows) and sloughed papillae (arrowheads),
consistent with severe papillary necrosis.
C, Axial unenhanced phase image was insufficient to make diagnosis.
A B C
Fig. 433-year-old woman with gross hematuria.
A and B, Axial (A) and sagittal (B) images from excretory phase of CT urogram show focal thickening (arrow, A) of anterior bladder wall at midline that
was considered suspicious for urothelial neoplasm. In retrospect, sagittal image (B) shows that area of thickening (arrowhead) is on serosal surface
and is contiguous with median umbilical ligament, finding typical of urachal insertion.
C, Finding was not evident on unenhanced image. Cystoscopy was deferred, and patient has had no genitourinary problems with 2 years of clinical follow-up.
rent urinalysis and urine culture revealed 50 There were nine findings in nine studies images that was not apparent on unenhanced
100 WBCs per high-power field and more than that were significant and required observa- images when the bladder was underdistend-
100,000 colonies of Escherichia coli. The tion, including four atrophic kidneys, two ed. The patient had a history of spinal cord
Downloaded from
second finding was heterogeneously di- neurogenic bladders, and one each of benign injury at the T2 level sustained during a mo-
minished enhancement of the right kidney, prostatic hyperplasia, interstitial cystitis, and tor vehicle collision in childhood. The pa-
which was suspicious for early or resolving papillary necrosis. Of these findings, seven tient with papillary necrosis had a history of
pyelonephritis in a patient with flank pain. The (77.8%) were detected on unenhanced im- multiple sclerosis, neurogenic bladder, and
patient had a history of obstructive urop-athy ages. One of two neurogenic bladders and recurrent urinary tract infections.
secondary to stone disease previously treated papillary necrosis (Fig. 3) required contrast- There were 68 findings in 66 studies that
with temporary ureteral stent place-ment. enhanced images for detection. The patient were clinically insignificant. The majori-ty
Urinalysis revealed 50100 WBCs, 2+ with neurogenic bladder had a thickened and were benign renal cortical cysts (n = 54
leukocyte esterase, and 4+ bacteria. trabeculated bladder wall on excretory phase [81.8%]). Forty-five (66.2%) of the insignifi-
612 AJR:198, March 2012
CT Urography to Evaluate Hematuria in Young Adults
ARRS. For personal use only; all rights reserved
A B C
Fig. 523-year-old man with multiple episodes of gross hematuria after long-distance running.
A and B, Axial (A) and sagittal (B) images from excretory phase CT urogram show focal thickening (arrows) of anterior bladder wall that was
considered suspicious for urothelial neoplasm.
C, Finding was not evident on unenhanced image. Cystoscopy and bladder wall biopsies obtained in region of CT abnormality showed benign urothelium.
cant findings were detected on unenhanced uation and hypoenhancement were reported as evaluation of adults with hematuria were
images alone. Seventeen benign cortical suspicious for pyelonephritis in a patient with published in 2001 and recommend initial
cysts, two patients with renal scarring, three bilateral cortical scarring and history of reflux upper urinary tract imaging with either ex-
duplicated renal collecting systems, and one nephropathy. The patient had no clinical symp- cretory urography or CT urography, in ad-
Downloaded from www.ajronline.org by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright
calyceal diverticulum required contrast-en- toms of pyelonephritis, and the findings were dition to cystoscopy of the urinary bladder
hanced images for diagnosis. more clearly shown to be blunted renal calyces and urine cytology [9]. Several studies have
Twelve genitourinary findings described in on a follow-up abdominal CT. A fluid-attenu- since shown increased detection of urinary
the radiology reports were found to be false- ating focus within the prostate was reported as calculi, renal masses, renal and perirenal in-
positive on clinical and radiologic follow-up. suspicious for prostatic abscess. A prostate ul- fections, and unsuspected extraurinary dis-
Suspected urothelial neoplasms of the blad-der trasound was recommended but deferred be- ease with CT urography compared with ex-
(n = 5) were followed by either negative cause of lack of clinical symptoms. cretory urography [2023]. CT urography is
cystoscopy (n = 2) or negative cystoscopy and Two additional false-positive findings were currently recommended over excretory
biopsy (n = 1) of the area of CT abnormal-ity. detected with unenhanced images. In one pa-tient, urog-raphy by the American College of
Cystoscopy was deferred in two of the pa- the right ureter took a reverse-J configura-tion Radiolo-gy in the evaluation of hematuria
tients. One of these patients had a history of thought to be suggestive of ureteral reflux. A [10] and is now used more often than
99m excretory urogra-phy by most
ketamine use at the time of the CT urogram. subsequent Tc mercaptoacetyltriglycine renal
The patient had an unenhanced CT scan 8 scintigram showed no associated abnor-mality. uroradiologists [15].
years later for recurrent hematuria, revealing One finding of suspected retroperitone-al fibrosis The recommendation that young adults
cystitis that was clinically attributed to contin- was stable on follow-up with two ad-ditional CT with microscopic hematuria be evaluated
ued ketamine use. The second patient had no urograms obtained over the next 9 months and with upper urinary tract imaging is support-
genitourinary problems after 2 years of clini- was later determined to represent tortuous ed by studies that discovered life-
cal follow-up. In retrospect, the CT finding in retroperitoneal vessels. threatening lesions on imaging [2427].
this patient was typical of an urachal inser-tion Three of the 375 CT urograms (0.8%) were However, sev-eral large studies have found
(Fig. 4). All suspected urothelial lesions of the associated with adverse events. One patient few clinical-ly significant lesions on
ureter (n = 2) were followed by nega-tive had a severe contrast material reaction that re- imaging of young adults with hematuria. In
ureteroscopy and retrograde pyelography (n = quired treatment with 0.3 mg of subcutaneous a retrospective study of 1000 Israeli Air
1) or retrograde pyelography alone (n = 1). epinephrine and subsequent monitoring in the Force personnel with asymptomatic
Four of the five suspected bladder lesions emergency department. One patient had a de- microscopic hematuria on routine annual
(80%) and two of the suspected ureteral le- layed contrast material reaction of facial swell- screening, Froom et al.
sions (100%) were visible only on the con- ing that was treated in the emergency depart- [3] detected malignancies in 0.1% of sub-
trast-enhanced images (Fig. 5). ment. One patient became anxious during IV jects, leading the authors to conclude that
Several additional false-positive findings catheter placement and experienced a presyn- asymptomatic microscopic hematuria may
were visible on contrast-enhanced images only. copal episode; after clinical evaluation in the not warrant urologic investigation in
An indeterminate solid-appearing renal lesion radiology department, the patient was treated patients younger than 40 years. Of 100
measuring 1.0 cm with equivocal enhancement with lorazepam. prospectively studied men aged 1640 years
was interpreted as a possible renal cell carcino- with micro-scopic hematuria, two
ma and remained stable in appearance on CT Discussion significant upper uri-nary tract lesions were
scans obtained up to 7 years after initial detec- Current best practice guidelines from the detected on excreto-ry urography, including
tion. Bilateral foci of renal cortical low atten- American Urologic Association for the one ureteral calculus and one duplex right
renal collecting system
[28]. Khadra et al. [13] prospectively stud-
ied 277 patients aged 40 years and younger
AJR:198, March 2012 613
Lokken et al.
who were referred to a hematuria clinic with patients with important findings missed on would have prompted additional contrast-en-
either gross or microscopic hematuria. Al- unenhanced images had significant predis- hanced imaging for further characterization;
though seven cases of bladder cancer were posing medical histories for urologic dis-ease, however, the majority of patients in our cohort
detected with cystoscopy, no upper urinary including prior malignancy, multiple sclerosis, would have been spared the additional radia-
tract malignancies were found on ultrasound spinal cord injury, history of re-current urinary tion dose associated with CT urography.
or excretory urography [13]. A prospective tract infections, or pyuria. Clinically Our findings should be interpreted in the
Downloaded from www.ajronline.org by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal use only; all rights reserved
study of 292 patients referred for asymptom- insignificant findings, most often renal cortical context of our study design and patient popu-
atic microscopic hematuria with 13 years of cysts of Bosniak category I or II, more often lation. Clinical information, including labora-
follow-up found no malignancies in patients required contrast-enhanced phase images for tory studies of patients referred to our hospi-tal
younger than 50 years on initial evaluation detection (n = 23/68 lesions [33.8%]). from outside institutions, was not always
[14]. The sensitivity of these studies may However, these findings affected neither available in the electronic medical record for
have been limited by evaluation of patients treatment nor prognosis and arguably did not confirmation. Because our patient population
with excretory urography or ultrasound in- require detection. In addition, many of these included a high proportion of patients who
stead of CT. In addition, the diagnostic yield findings may have been coinciden-tal rather were referred to urologists, our recommenda-
may have been further limited in several than causative of hematuria, as has been long tions should be applied with caution to young
studies by the use of a screened sample of stressed in the literature [30]. adult patients with hematuria evaluated in the
the general population instead of a referred Our findings support current guidelines that primary care setting, who may have a lower
population [29]. Several of these studies re- recommend imaging of the upper uri-nary tract pretest probability of significant urologic dis-
ported only malignant lesions instead of all of young patients with gross or microscopic ease [29]. The European Society of Urogeni-tal
findings likely to affect patient management. hematuria but raise questions as to whether CT Radiology recommends ultrasound as the
In the present study, CT urography yield- urography is the optimal modality for imaging primary imaging test in patients younger than
ed a clinically significant diagnosis in 22.1% evaluation. Given the high prevalence of 40 years with either microscopic or gross he-
of young adult patients with gross or micro- urinary tract calculi and the detection of maturia [32]. It is possible that our cohort in-
scopic hematuria. The majority (75.3%) of several renal and perirenal masses, our data cluded patients who were prescreened with
clinically significant findings were renal or support the use of CT over excretory ultrasound, which may further reduce the
ureteral calculi. However, we also detected urography [23, 31]. However, our findings findings missed by using unenhanced CT
malignancies in four patients. All tumors suggest that the majority of young adults with alone. Finally, only axial unenhanced images
were renal or perirenal masses, with no con- hematuria could be optimally evaluated with a were available for evaluation by our blinded
firmed urothelial lesions detected. single phase unenhanced CT, reserving CT reviewer. Because of the lack of sagittal and
CT urography also resulted in adverse urography for patients with significant coronal reformations, which are customar-ily
outcomes for several patients in the form of predisposing conditions for uro-logic disease in included in single phase unenhanced CT
false-positive findings and contrast agent addition to hematuria. This imaging strategy studies of the urinary tract at many institu-
reactions. The majority (n = 7 [58.3%]) of the would have allowed detec-tion of all clinically tions, we may have underestimated the diag-
12 false-positive findings were suspect-ed significant urologic le-sions in our cohort and nostic yield of unenhanced images for uro-
urothelial lesions of the ureters or uri-nary may have reduced de-tection of false-positive logic findings.
bladder, with no true-positive urotheli-al findings by 75.0%. In conclusion, the yield of CT urography
lesions detected. Workup of false-positive The increasing use of CT urography as the for significant urologic disease was 22.1%
findings resulted in seven unnecessary CT initial imaging test raises concerns about ra- in young adults imaged for hematuria. How-
studies, one ureteroscopy, one bladder biop-sy, diation exposure. It has been estimated that ever, a single phase unenhanced CT may be
two retrograde pyelograms, one cystosco- 0.4% of all cancers in the United States may be sufficient for the majority of these patients
py that would otherwise have been deferred, attributable to radiation from CT stud-ies, with without additional predisposing medical
99m the lifetime attributable risk of can-cer death con-ditions. These data will help determine
and one Tc mercaptoacetyltriglycine
renal scintigram. The ureteroscopy was increasing in patients younger than 40 years the appropriate indications for CT urography
compli-cated by ureteral injury, resulting in [17]. The mean effective dose of CT urography in patients with hematuria.
tempo-rary ureteral stent placement, three of 14.8 mSv leads to approximate-ly 1.5 times
visits to the emergency department, and one the radiation risk from excretory urography; in Acknowledgment
hospital admission. In addition, three addition, when a two-scan split-bolus CT We thank Jorge Fuentes Orrego for his
patients (0.8%) experienced adverse contrast urography protocol with dose modu-lation is contribution to data acquisition.
material reac-tions, of which two required used, the mean effective dose of CT urography
treatment in the emergency department. is twice that of a single phase CT References
The majority of findings in our study, in- [16]. Given the relatively high radiation dose 1. Chen BT, Ooi BS, Tan KK, Lim CH. Comparative
cluding 92 (94.8%) of the 97 clinically signif- of multiphase CT urography, an alternative studies of asymptomatic proteinuria and hematu-ria.
icant findings, were evident on unenhanced imaging strategy that includes unenhanced CT Arch Intern Med 1974; 134:901905
images. The five important lesions that were for the majority of patients would substantial- 2. Mohr DN, Offord KP, Owen RA, Melton LJ.
missed on unenhanced images included lym- ly reduce radiation exposure to this radiosen- Asymptomatic microhematuria and urologic dis-
phomatous involvement of the kidney, pyelo- sitive population. Several findings detected on ease: a population-based study. JAMA 1986;
nephritis, bacterial cystitis, neurogenic blad- unenhanced images in our study, such as sus- 256:224229
der, and papillary necrosis. However, all five pected ureteral transection and a renal mass, 3. Froom P, Ribak J, Benbassat J. Significance of mi-
614 AJR:198, March 2012
CT Urography to Evaluate Hematuria in Young Adults
crohaematuria in young adults. Br Med J (Clin Kumazawa J. Clinical study of asymptomatic mi- study. J Urol 2004; 171:237243
Res Ed) 1984; 288:2022 croscopic haematuria. Int Urol Nephrol 1994; 22. Liu W, Mortele KJ, Silverman SG. Incidental ex-
4. Buntinx F, Wauters H. The diagnostic value of 26:16 traurinary findings at MDCT urography in pa-
macroscopic haematuria in diagnosing urological 13. Khadra MH, Pickard RS, Charlton M, Powell tients with hematuria: prevalence and impact on
cancers: a meta-analysis. Fam Pract 1997; PH, Neal DE. A prospective analysis of 1,930 imaging costs. AJR 2005; 185:10511056
14:63 68 patients with hematuria to evaluate current 23. Albani JM, Ciaschini MW, Streem SB, Herts BR,
Downloaded from www.ajronline.org by 115.178.238.12 on 09/26/17 from IP address 115.178.238.12. Copyright ARRS. For personal use only; all rights reserved
5. Grossfeld GD, Carroll PR. Evaluation of asymp- diagnostic practice. J Urol 2000; 163:524527 Angermeier KW. The role of computerized tomo-
tomatic microscopic hematuria. Urol Clin North 14. Mishriki SF, Nabi G, Cohen NP. Diagnosis of uro- graphic urography in the initial evaluation of he-
Am 1998; 25:661676 logic malignancies in patients with asymptomatic maturia. J Urol 2007; 177:644648
6. Sanders C. Clinical urine examination and the in- dipstick hematuria: prospective study with 13 years 24. Gartman E. The significance of hematuria in
cidence of microscopic haematuria in apparently follow-up. Urology 2008; 71:1316 young men. J Urol 1956; 75:135142
normal males. Practitioner 1963; 191:192197 15. Townsend BA, Silverman SG, Mortele KJ, Tun- 25. Carson CC, Segura JW, Greene LF. Clinical im-
7. Woolhandler S, Pels RJ, Bor DH, Himmelstein cali K, Cohan RH. Current use of computed portance of microhematuria. JAMA 1979;
DU, Lawrence RS. Dipstick urinalysis screening tomo-graphic urography: survey of the society of 241:149150
of asymptomatic adults for urinary tract disor- urora-diology. J Comput Assist Tomogr 2009; 26. Ritchie CD, Bevan EA, Collier SJ. Importance of
ders. Part I. Hematuria and proteinuria. JAMA 33:96100 occult haematuria found at screening. Br Med J
1989; 262:12141219 16. Nawfel RD, Judy PF, Schleipman AR, Silverman (Clin Res Ed) 1986; 292:681683
8. Grossfeld GD, Litwin MS, Wolf JS Jr, et al. Evalu- SG. Patient radiation dose at CT urography and 27. Mariani AJ, Mariani MC, Macchioni C, Stams
ation of asymptomatic microscopic hematuria in conventional urography. Radiology 2004; UK, Hariharan A, Moriera A. The significance of
adults: the American Urological Association best 232:126132 adult hematuria: 1,000 hematuria evaluations in-
practice policy. Part I. Definition, detection, prev- 17. Brenner DJ, Hall EJ. Computed tomography: an cluding a risk-benefit and cost-effectiveness anal-
alence, and etiology. Urology 2001; 57:599603 increasing source of radiation exposure. N Engl J ysis. J Urol 1989; 141:350355
9. Grossfeld GD, Litwin MS, Wolf JS Jr, et al. Med 2007; 357:22772284 28. Jones DJ, Langstaff RJ, Holt SD, Morgans BT.
Evalu-ation of asymptomatic microscopic 18. Silverman SG, Akbar SA, Mortele KJ, Tuncali K, The value of cystourethroscopy in the investiga-
hematuria in adults: the American Urological Bhagwat JG, Seifter JL. Multi-detector row CT tion of microscopic haematuria in adult males
Association best practice policy. Part II. Patient urography of normal urinary collecting system: under 40 years: a prospective study of 100 pa-
evaluation, cytol-ogy, voided markers, imaging, furosemide versus saline as adjunct to contrast tients. Br J Urol 1988; 62:541545
cystoscopy, ne-phrology evaluation, and follow- medium. Radiology 2006; 240:749755 29. Sutton JM. Evaluation of hematuria in adults.
up. Urology 2001; 57:604610 19. Chow LC, Kwan SW, Olcott EW, Sommer G. JAMA 1990; 263:24752480
10. American College of Radiology. ACR Appropri- Split-bolus MDCT urography with synchronous 30. Greene LF, OShaughnessy EJ Jr, Hendricks ED.
ateness Criteria: hematuria. American College of nephrographic and excretory phase enhancement. Study of five hundred patients with asymptomatic
Radiology Website. www.acr.org/Secondary- AJR 2007; 189:314322 microhematuria. JAMA 1956; 161:610613
MainMenuCategories/quality_safety/app_crite- 20. Gray Sears CL, Ward JF, Sears ST, Puckett MF, 31. Fielding JR, Silverman SG, Samuel S, Zou KH,
ria/pdf/ExpertPanelonUrologicImaging/Hematu- Kane CJ, Amling CL. Prospective comparison of Loughlin KR. Unenhanced helical CT of ureteral
riaDoc6.aspx. Published 1995. Updated 2008. computerized tomography and excretory urogra- stones: a replacement for excretory urography in
Accessed May 15, 2011 phy in the initial evaluation of asymptomatic mi- planning treatment. AJR 1998; 171:10511053
11. Woodhouse CR. Symptomless abnormalities: mi- crohematuria. J Urol 2002; 168:24572460 32. Van Der Molen AJ, Cowan NC, Mueller-Lisse
croscopic haematuria. Br J Hosp Med 1982; 21. Lang EK, Thomas R, Davis R, et al. Multiphasic UG, et al. CT urography: definition, indications,
27:163168 helical computerized tomography for the assess- and techniques: a guideline for clinical practice.
12. Yasumasu T, Koikawa Y, Uozumi J, Ueda T, ment of microscopic hematuria: a prospective Eur Radiol 2008; 18:417
AJR:198, March 2012 615
You might also like
- Jadwal Neuro WekwekDocument2 pagesJadwal Neuro WekwekAnthonyJohanNo ratings yet
- 1 PBDocument8 pages1 PBAnthonyJohanNo ratings yet
- Status Ujian (1) AjDocument6 pagesStatus Ujian (1) AjAnthonyJohanNo ratings yet
- Management of Malignant Hyperthermia: Diagnosis and TreatmentDocument5 pagesManagement of Malignant Hyperthermia: Diagnosis and TreatmentAnthonyJohanNo ratings yet
- Brain Sciences: A Double-Edged Sword: Volatile Anesthetic Effects On The Neonatal BrainDocument22 pagesBrain Sciences: A Double-Edged Sword: Volatile Anesthetic Effects On The Neonatal BrainAnthonyJohanNo ratings yet
- Case Series Article 2014Document22 pagesCase Series Article 2014AnthonyJohanNo ratings yet
- Mechanisms of Disease Alterations in Body Defenses: Unit OneDocument4 pagesMechanisms of Disease Alterations in Body Defenses: Unit OneAnthonyJohanNo ratings yet
- Hipotiroid Kongenital - MedscapeDocument15 pagesHipotiroid Kongenital - MedscapeAnthonyJohanNo ratings yet
- 92 FullDocument9 pages92 FullAnthonyJohanNo ratings yet
- Translating Vascular Biology Into Clinical Care For Cardiology K .MaieseDocument1 pageTranslating Vascular Biology Into Clinical Care For Cardiology K .MaieseAnthonyJohanNo ratings yet
- DocumentDocument7 pagesDocumentdewiNo ratings yet
- PearsonsDocument8 pagesPearsonsalparselanNo ratings yet
- Faktor Risiko Hipertensi Intradialitik Pasien Penyakit Ginjal KronikDocument16 pagesFaktor Risiko Hipertensi Intradialitik Pasien Penyakit Ginjal KronikAnthonyJohanNo ratings yet
- Arena Guide - Icy VeinsDocument10 pagesArena Guide - Icy VeinsAnthonyJohanNo ratings yet
- Practice Guidelines For AcupuncturistsDocument9 pagesPractice Guidelines For AcupuncturistsAnthonyJohanNo ratings yet
- Emerg Med J 2003 Mann 54 60Document8 pagesEmerg Med J 2003 Mann 54 60dnnivNo ratings yet
- TriageDocument4 pagesTriageAnthonyJohanNo ratings yet
- IDWG marker BP, nutrition, survival HDDocument6 pagesIDWG marker BP, nutrition, survival HDAnthonyJohanNo ratings yet
- Build PropDocument15 pagesBuild PropAnthonyJohan100% (1)
- Diabetes + CKD PDFDocument8 pagesDiabetes + CKD PDFAmelia GustinNo ratings yet
- CKD InfoDocument20 pagesCKD Infotheboy14juneNo ratings yet
- Hemothorax - MedscapeDocument14 pagesHemothorax - MedscapeAnthonyJohanNo ratings yet
- Blunt and Penetrating Trauma - MedscapeDocument29 pagesBlunt and Penetrating Trauma - MedscapeAnthonyJohanNo ratings yet
- ReleaseDocument1 pageReleaseGabriel StoicaNo ratings yet
- Ske 2 - Drowning MedscapeDocument20 pagesSke 2 - Drowning MedscapeAnthonyJohanNo ratings yet
- Insulin BasicsDocument6 pagesInsulin BasicsAnthonyJohanNo ratings yet
- Ske 2 - Drowning MedscapeDocument20 pagesSke 2 - Drowning MedscapeAnthonyJohanNo ratings yet
- Hemothorax - MedscapeDocument14 pagesHemothorax - MedscapeAnthonyJohanNo ratings yet
- Exhaled 8-Isoprostane As An Biomarker of Lung Oxidative Stress in Patients With COPD and Healthy SmokersDocument3 pagesExhaled 8-Isoprostane As An Biomarker of Lung Oxidative Stress in Patients With COPD and Healthy SmokersAnthonyJohanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Eau Guidelines On Urological Infections: (Limited Text Update March 2022)Document27 pagesEau Guidelines On Urological Infections: (Limited Text Update March 2022)Andrea Romano ForcinitiNo ratings yet
- Common Illnesses and Classique ProductsDocument52 pagesCommon Illnesses and Classique Productsmj_jm255114100% (1)
- Urine Characteristics & UrinalysisDocument30 pagesUrine Characteristics & UrinalysisiwennieNo ratings yet
- Benign Prostatic HyperplasiaDocument9 pagesBenign Prostatic Hyperplasiamardsz100% (1)
- ATI Comprehensive & MentalDocument998 pagesATI Comprehensive & MentalYolanda Stark96% (45)
- Bachelor of Science in Nursing:: Course Module Course Unit WeekDocument8 pagesBachelor of Science in Nursing:: Course Module Course Unit WeekMaye ArugayNo ratings yet
- Chapter 66 Care of Patients With Urinary ProblemsDocument11 pagesChapter 66 Care of Patients With Urinary ProblemsGina GiammalvoNo ratings yet
- Clinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenDocument8 pagesClinical Practice Guideline on Approach and Treatment of Urinary Tract Infection in ChildrenPaula QuiñonesNo ratings yet
- Urikind Tablet Uses - Google SearchDocument1 pageUrikind Tablet Uses - Google SearchPushpa TimmapurNo ratings yet
- Hyperbaric Soft Tissue RadionecrosisDocument13 pagesHyperbaric Soft Tissue Radionecrosisina permata dewiNo ratings yet
- Understanding Urine AnalysisDocument3 pagesUnderstanding Urine AnalysisDarius June Nolasco SacupasoNo ratings yet
- Odessa National Medical University: Surgical InfectionsDocument34 pagesOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriNo ratings yet
- Genito-Urinary System and Disorders - RATIONALIZATIONDocument6 pagesGenito-Urinary System and Disorders - RATIONALIZATIONCarlo Paul Castro SanaNo ratings yet
- Post Mortem Examination Renal SystemDocument17 pagesPost Mortem Examination Renal SystemDanNo ratings yet
- Urology For Medical Student Hora 19-12-2008Document77 pagesUrology For Medical Student Hora 19-12-2008Adriana SantosNo ratings yet
- OB Intern's Review - Dra LeeDocument214 pagesOB Intern's Review - Dra LeeKathleenZunigaNo ratings yet
- 6 Daftar Pustaka KTI MIKRO Sri Hayati Revisi 2Document3 pages6 Daftar Pustaka KTI MIKRO Sri Hayati Revisi 2Sri Hayati NufalianaNo ratings yet
- TantraDocument13 pagesTantraapi-26231809No ratings yet
- Aafp Uti GuidelinesDocument10 pagesAafp Uti GuidelinesCess Lagera YbanezNo ratings yet
- Possible Interview Questions For NursesDocument32 pagesPossible Interview Questions For NursesElisabeta Ivan75% (4)
- Urine Investigations SmiDocument51 pagesUrine Investigations SmiAnXa Ali JanJuaNo ratings yet
- Zinnat - Suspension GDS27 IPI07Document7 pagesZinnat - Suspension GDS27 IPI07Kim RNo ratings yet
- Bladder DiverticulaDocument23 pagesBladder DiverticulaJeanette CallejasNo ratings yet
- NorvisDocument3 pagesNorvisWilliam LieNo ratings yet
- Back Pain History TakingDocument4 pagesBack Pain History TakingAmjad_2020No ratings yet
- CH 20 Nursing Care of A Family Experiencing A Pregnancy ComplicationDocument18 pagesCH 20 Nursing Care of A Family Experiencing A Pregnancy Complicationcutiepie creampieNo ratings yet
- Gram-Negative Bacteria Diseases and TreatmentsDocument4 pagesGram-Negative Bacteria Diseases and TreatmentswingNo ratings yet
- UTI in PregnancyDocument33 pagesUTI in Pregnancyyusufkiduchu8No ratings yet
- EAU Guidelines On Paediatric Urology 2018 Large TextDocument159 pagesEAU Guidelines On Paediatric Urology 2018 Large Textamandashn96100% (1)
- MS and Me: A Self-Management Guide To Living With MSDocument44 pagesMS and Me: A Self-Management Guide To Living With MSDeepaNo ratings yet