You might also like
- Leadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Document38 pagesLeadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Mack MakaNo ratings yet
- Medication Errors FinalDocument7 pagesMedication Errors Finalapi-469407326No ratings yet
- PoliomyelitisDocument57 pagesPoliomyelitisPradnya Warthe100% (1)
- PCOSDocument4 pagesPCOSTp HoangNo ratings yet
- Unequal Distribution of Health Services Biggest Global Health ProblemDocument3 pagesUnequal Distribution of Health Services Biggest Global Health ProblemHaleemaMunir0% (1)
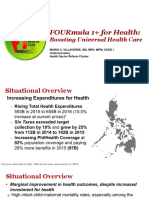
- 4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoDocument12 pages4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoJanella DandanNo ratings yet
- Chapter 32: Nursing Care of A Family With A School-Aged ChildDocument10 pagesChapter 32: Nursing Care of A Family With A School-Aged ChildJordan GougerNo ratings yet
- POLIOMYELITISDocument26 pagesPOLIOMYELITISIzhra Margate100% (1)
- CHN Health PromotionDocument7 pagesCHN Health PromotionNareeza AbdullaNo ratings yet
- Challenges in NursingDocument4 pagesChallenges in NursingAnju PandeyNo ratings yet
- A. As A Nurse, How Do You Develop Your Critical Thinking?Document17 pagesA. As A Nurse, How Do You Develop Your Critical Thinking?Princess Melanie MelendezNo ratings yet
- NEUST College of Nursing Exam on Communicable DiseasesDocument3 pagesNEUST College of Nursing Exam on Communicable DiseasesJohn Eldrin LaureanoNo ratings yet
- Observation Report - Hemodialysis - Kit P. RoaquinDocument15 pagesObservation Report - Hemodialysis - Kit P. Roaquineljhayar_18No ratings yet
- Final ResearchDocument65 pagesFinal ResearchHarbrinder GurmNo ratings yet
- Change ProjectDocument10 pagesChange ProjectMartin ManaluNo ratings yet
- IMCI Chart BookletDocument39 pagesIMCI Chart Bookletкristina YambaNo ratings yet
- Health Education PlanDocument1 pageHealth Education PlanSheena ClaireNo ratings yet
- "Why Did You Decide On A Career As A Nurse?": Example AnswerDocument3 pages"Why Did You Decide On A Career As A Nurse?": Example AnswerAnita DewiNo ratings yet
- Health Care Delivery SystemDocument42 pagesHealth Care Delivery SystemDr. Jayesh Patidar100% (1)
- The First Ever Application Based Drug Delivery Service "MED-DEL"Document17 pagesThe First Ever Application Based Drug Delivery Service "MED-DEL"Khaled Bin Shahabuddin ShagarNo ratings yet
- Learning PlanDocument5 pagesLearning PlansameenaesmailNo ratings yet
- CH 20 Nursing Care of Patients With HIVDocument2 pagesCH 20 Nursing Care of Patients With HIVZachary T Hall100% (1)
- Nursing Jurisprudence - For UploadDocument290 pagesNursing Jurisprudence - For UploadBing58No ratings yet
- Vitamin CDocument18 pagesVitamin CMarcel Gloria PongendaNo ratings yet
- Survey Emotional IntelligenceDocument2 pagesSurvey Emotional IntelligenceJohanna Estacion BibitNo ratings yet
- Shortage of StaffDocument5 pagesShortage of Staffapi-314555733No ratings yet
- Professional Role Development Plan NewDocument8 pagesProfessional Role Development Plan Newapi-532226029No ratings yet
- Assessing Family Health NeedsDocument5 pagesAssessing Family Health NeedsRodolf Gerone G. MacahilosNo ratings yet
- CHN Notes For MidtermsDocument24 pagesCHN Notes For MidtermsReiner Lopez100% (1)
- Acute Urinary RetentionDocument14 pagesAcute Urinary RetentionTP RMadNo ratings yet
- Geriatric Dehydration EducationDocument14 pagesGeriatric Dehydration EducationJ Therese NorrellNo ratings yet
- Copar Process ModuleDocument5 pagesCopar Process ModuleMrs RehanNo ratings yet
- Types of Anemia ExplainedDocument8 pagesTypes of Anemia ExplainedApril Mae Magos LabradorNo ratings yet
- Patient Centred Clinical Method GuideDocument44 pagesPatient Centred Clinical Method GuideBeLovedOneTooNo ratings yet
- Ebp Synthesis PaperDocument8 pagesEbp Synthesis Paperapi-404285262No ratings yet
- Nursing ProcessDocument5 pagesNursing ProcessStacy CamposNo ratings yet
- Hepatitis BDocument12 pagesHepatitis BTeti AndriNo ratings yet
- CVDisease NUTRIDocument30 pagesCVDisease NUTRIMariano Marbella100% (1)
- Prof. Maria Susan Z. MaglaquiDocument24 pagesProf. Maria Susan Z. MaglaquiSusan MaglaquiNo ratings yet
- The Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGDocument7 pagesThe Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGSabhi Sandhu100% (1)
- Essential Guide to Cerebral PalsyDocument36 pagesEssential Guide to Cerebral PalsyLeigh Ann Prosyne LozadaNo ratings yet
- NCMB 419 Week 11 CU10Document23 pagesNCMB 419 Week 11 CU10GERALDINE GONZALESNo ratings yet
- Ipsg 6 Patient SafetyDocument12 pagesIpsg 6 Patient SafetyJamilaturRasyidahEfendiNo ratings yet
- Aminoglycoside Antibiotics Mechanism, Uses and ToxicityDocument2 pagesAminoglycoside Antibiotics Mechanism, Uses and ToxicityمحمدأميندماجNo ratings yet
- Planning of Nursing ProcessDocument14 pagesPlanning of Nursing ProcessJoviNo ratings yet
- Research in Nursing: A Quest for KnowledgeDocument146 pagesResearch in Nursing: A Quest for KnowledgeHanna JalemNo ratings yet
- Time Management Strategies in PracticeDocument9 pagesTime Management Strategies in PracticeAnke Nemirovsky100% (1)
- NCM 107-A Nursing Leadership & Management ConceptsDocument241 pagesNCM 107-A Nursing Leadership & Management ConceptsMichael Anthony Ermita50% (2)
- NCM104b BSN220 Mobility NursingDocument9 pagesNCM104b BSN220 Mobility NursingChristian Apelo SerquillosNo ratings yet
- Phases of The COPAR ProcessDocument8 pagesPhases of The COPAR ProcessmerlNo ratings yet
- Influenza Health Promotion ProjectDocument8 pagesInfluenza Health Promotion Projectapi-284269118No ratings yet
- 9 Tips On How To Make A Good SOAPIEDocument7 pages9 Tips On How To Make A Good SOAPIEMagbanua Airene MarielNo ratings yet
- Post-op Nursing Care GuideDocument12 pagesPost-op Nursing Care GuideAhmed AliNo ratings yet
- Professional Development PlanDocument2 pagesProfessional Development Planapi-578003485No ratings yet
- CM1, CU 1, WK 1-Introduction To Leadership and ManagementDocument16 pagesCM1, CU 1, WK 1-Introduction To Leadership and ManagementMichelle Gliselle Guinto MallareNo ratings yet
- Cardiac Surgery Patient Case StudyDocument14 pagesCardiac Surgery Patient Case StudyNana YaaNo ratings yet
- DischargeDocument49 pagesDischargejonel_amarilleNo ratings yet
- Postoperative Care for Patients with Cardiovascular and Renal IssuesDocument6 pagesPostoperative Care for Patients with Cardiovascular and Renal IssuesAziil LiizaNo ratings yet
- A. Discussion of The Health ConditionDocument5 pagesA. Discussion of The Health ConditionPeter AbellNo ratings yet
- Gnur 405 SuzyDocument6 pagesGnur 405 SuzySeth MensahNo ratings yet
- TCA CrossDocument6 pagesTCA CrosssalivaNo ratings yet
- Just Culture CommissionDocument27 pagesJust Culture CommissionAlina PetichenkoNo ratings yet
- Sarnat 1976Document10 pagesSarnat 1976João Paulo RaposoNo ratings yet
- Thyroid CytologyDocument36 pagesThyroid CytologyNaglaa RamadanNo ratings yet
- Shaken Baby SyndromeDocument25 pagesShaken Baby SyndromeArdanta Dat Topik TariganNo ratings yet
- 2019 Quality Metrics For The Evaluation of Rapid Response SystemsDocument12 pages2019 Quality Metrics For The Evaluation of Rapid Response Systemsbogeg74816No ratings yet
- Learning Objective: - Explain of Acute AbdomenDocument143 pagesLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiNo ratings yet
- Stigma in PsihozaDocument22 pagesStigma in PsihozaBurca LarisaNo ratings yet
- Alcohol Binge Drinking in OCDDocument2 pagesAlcohol Binge Drinking in OCDSuyash DwivediNo ratings yet
- Nutrition diagnosis: Imbalanced nutrition less than requirementsDocument3 pagesNutrition diagnosis: Imbalanced nutrition less than requirementsIlisa ParilNo ratings yet
- CBTDocument2 pagesCBTSHAH JAHAN BANONo ratings yet
- Lip Augmentation, Lip Reduction, and Lip Lift Niamtu PDFDocument75 pagesLip Augmentation, Lip Reduction, and Lip Lift Niamtu PDFAbdullah özel100% (1)
- Internal Medicine Write Up 1Document16 pagesInternal Medicine Write Up 1Ariff MahdzubNo ratings yet
- Critical Care Testing - Quality AssuranceDocument120 pagesCritical Care Testing - Quality AssuranceAbhijit Mokashi100% (1)
- Universal Precautions PPT FinalDocument50 pagesUniversal Precautions PPT Finalmarthinfp100% (1)
- Obesity Is The Most Nutritional Among Children Developed CountriesDocument14 pagesObesity Is The Most Nutritional Among Children Developed CountriesBulanBiruNo ratings yet
- Pomr 1Document7 pagesPomr 1Afifa Prima GittaNo ratings yet
- Foot and Ankle Clinics Volume A Refined Classification SystemDocument17 pagesFoot and Ankle Clinics Volume A Refined Classification SystemRicardo CastilloNo ratings yet
- Diverticulosis!!Document10 pagesDiverticulosis!!Nahdah AidahNo ratings yet
- Acute Mild Traumatic Brain Injury (Concussion) in Adults - UpToDateDocument22 pagesAcute Mild Traumatic Brain Injury (Concussion) in Adults - UpToDateZulvina FaozanudinNo ratings yet
- Soft tissue closure techniques for oroantral communicationsDocument9 pagesSoft tissue closure techniques for oroantral communicationsLalo DmNo ratings yet
- Natural Cure CenterDocument7 pagesNatural Cure CenterNandhini ArunNo ratings yet
- Unit 1 - Ways Informatics Transforming Health CareDocument22 pagesUnit 1 - Ways Informatics Transforming Health CareRaquel MonsalveNo ratings yet
- Testing Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesDocument11 pagesTesting Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesJosé Carlos Sánchez-RamirezNo ratings yet
- Acute Flaccid ParalysisDocument4 pagesAcute Flaccid ParalysisZharah RuzNo ratings yet
- Oxygen-Induced Hypercapnia in COPD PDFDocument4 pagesOxygen-Induced Hypercapnia in COPD PDFsatyagraha84No ratings yet
- Eob2 Drug PDFDocument2 pagesEob2 Drug PDFBayu PrabowoNo ratings yet
- PROSTHODONTICS SEMINAR II Topics 1Document1 pagePROSTHODONTICS SEMINAR II Topics 1Jalil Enock0% (1)
- Mental Health of Older Adults: Facts, Risks & WHO ResponseDocument6 pagesMental Health of Older Adults: Facts, Risks & WHO Responsesergius3No ratings yet
- Bisphenol A Epoxy ResinDocument1 pageBisphenol A Epoxy ResincnhathoangNo ratings yet