You might also like
- AIS2 DR Daniel Nuzum Hormoneclass Detox ProtocolDocument24 pagesAIS2 DR Daniel Nuzum Hormoneclass Detox ProtocolPanther Prime50% (2)
- Dokumen - Tips - Detoxification Healing Dietrich KlinghardtDocument23 pagesDokumen - Tips - Detoxification Healing Dietrich KlinghardtakiniramNo ratings yet
- Tongue Diagnosis of Traditional Chinese Medicine For Rheumatoid ArthritisDocument19 pagesTongue Diagnosis of Traditional Chinese Medicine For Rheumatoid Arthritisluyawin100% (1)
- Gold Refining by Solvent Extraction-The Minataur™ ProcessDocument6 pagesGold Refining by Solvent Extraction-The Minataur™ ProcessahmedkhidryagoubNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 16: HematologyFrom EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyNo ratings yet
- Alpha Male Training The Secret That Doubles Testosterone Book PDFDocument16 pagesAlpha Male Training The Secret That Doubles Testosterone Book PDFDean RogersNo ratings yet
- Trace Elements: Reed A Berger MD Visiting Clinical Professor in NutritionDocument47 pagesTrace Elements: Reed A Berger MD Visiting Clinical Professor in NutritionGramoz CubreliNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- ArchRheumatol 32 21Document5 pagesArchRheumatol 32 21indriNo ratings yet
- Serum Oxidative Stress Markers Are Not Associated With Renal and Common Carotid Arteries Arteriosclerotic Vascular Changes in Patients With GoutDocument7 pagesSerum Oxidative Stress Markers Are Not Associated With Renal and Common Carotid Arteries Arteriosclerotic Vascular Changes in Patients With GoutTeodorNo ratings yet
- Research Paper: 10 Ml/min DecreaseDocument11 pagesResearch Paper: 10 Ml/min DecreaseRizka Nurul FirdausNo ratings yet
- Comparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaDocument7 pagesComparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaInternational Organization of Scientific Research (IOSR)No ratings yet
- Association of Admission Serum Calcium Levels and in Hospital Mortality in Patients With Acute ST Elevated Myocardial InfarctionDocument7 pagesAssociation of Admission Serum Calcium Levels and in Hospital Mortality in Patients With Acute ST Elevated Myocardial InfarctionMarcellia AngelinaNo ratings yet
- Splenectomy Is A Risk Factor For Developing Hyperuricemia and Nephrolithiasis in PDFDocument3 pagesSplenectomy Is A Risk Factor For Developing Hyperuricemia and Nephrolithiasis in PDFDayanne TeixeiraNo ratings yet
- Serum Mercury Level and Multiple SclerosisDocument4 pagesSerum Mercury Level and Multiple SclerosisMirza RisqaNo ratings yet
- Research ArticleDocument9 pagesResearch ArticlemikeNo ratings yet
- Impairment of Bone Health in Pediatric Patients With Hemolytic AnemiaDocument7 pagesImpairment of Bone Health in Pediatric Patients With Hemolytic AnemiaMarifer EstradaNo ratings yet
- Accumulation of Cells With Short Telomeres Is Associated With Impaired Zinc Homeostasis and Infl Ammation in Old Hypertensive ParticipantsDocument7 pagesAccumulation of Cells With Short Telomeres Is Associated With Impaired Zinc Homeostasis and Infl Ammation in Old Hypertensive ParticipantsGabriela Elizabeth Delgado LeijaNo ratings yet
- Ojsadmin, 7Document7 pagesOjsadmin, 7Veronika WijayaNo ratings yet
- A Study of Serum For Calcium and Ra Factor in Patients Undergoing Rheumatoid ArthritisDocument14 pagesA Study of Serum For Calcium and Ra Factor in Patients Undergoing Rheumatoid ArthritisInternational Journal of Innovative Science and Research Technology100% (2)
- Relation of Iron Status To Prognosis After Acute Coronary SyndromeDocument9 pagesRelation of Iron Status To Prognosis After Acute Coronary SyndromeselvianaNo ratings yet
- Laboratory Features of Systemic Lupus Erythematosus (SLE)Document6 pagesLaboratory Features of Systemic Lupus Erythematosus (SLE)AmrKamalNo ratings yet
- BloodDocument9 pagesBloodGek IwikNo ratings yet
- Chen 2013Document6 pagesChen 2013malaNo ratings yet
- 012 Analysis of Reticulocyte Parameters On The Sysmex XEDocument8 pages012 Analysis of Reticulocyte Parameters On The Sysmex XEblanket_thNo ratings yet
- Tugas Jurnal KardioDocument5 pagesTugas Jurnal KardioKiki AmandaNo ratings yet
- Kuliah Path Clin MSK 2017Document26 pagesKuliah Path Clin MSK 2017LioraNo ratings yet
- Prolong Storage of Blood in EDTADocument5 pagesProlong Storage of Blood in EDTAGriffin MulofwaNo ratings yet
- Admin, Ahmad MulyadiDocument6 pagesAdmin, Ahmad MulyadiDinda SaviraNo ratings yet
- The Role of The Platelet-To-Lymphocyte Ratio and NDocument5 pagesThe Role of The Platelet-To-Lymphocyte Ratio and NRudy Arindra WijayaNo ratings yet
- Serum Uric Acid As A Potential Biomarker in PatienDocument19 pagesSerum Uric Acid As A Potential Biomarker in PatienEfen YtNo ratings yet
- Elemental Analysis of Blood in Oral Cancer: T R Rautray, V Vijayan PkhotaDocument5 pagesElemental Analysis of Blood in Oral Cancer: T R Rautray, V Vijayan PkhotatapashrautrayNo ratings yet
- Reticulocyte Parameters: Why Should Clinical Laboratories Evaluate and Report Them?Document2 pagesReticulocyte Parameters: Why Should Clinical Laboratories Evaluate and Report Them?EvainoirNo ratings yet
- 8 T - Say - / - WH @ucqr - /yb)Document5 pages8 T - Say - / - WH @ucqr - /yb)Meilia Ayu SuariNo ratings yet
- Red Blood Cell Lipids, Serum Trace Elements and Immunological Markers in Prostatic Disease Patients An Investigative StudyDocument8 pagesRed Blood Cell Lipids, Serum Trace Elements and Immunological Markers in Prostatic Disease Patients An Investigative StudyEditor IJTSRDNo ratings yet
- Larussa 2017Document25 pagesLarussa 2017alan.rangel.puenteNo ratings yet
- Case Reports of RhupusDocument4 pagesCase Reports of RhupusSalwiyadiNo ratings yet
- 2012 The Effects of Medical Ozone Therapy On Renal Ischemia:Reperfusion InjuryDocument6 pages2012 The Effects of Medical Ozone Therapy On Renal Ischemia:Reperfusion InjuryAcupuntura de EquinosNo ratings yet
- The Journal of Rheumatology Volume 42, No. 7Document7 pagesThe Journal of Rheumatology Volume 42, No. 7salclNo ratings yet
- Dwivedi 2015Document7 pagesDwivedi 2015daypranitaNo ratings yet
- Kinsella Mia Fracture RiskDocument6 pagesKinsella Mia Fracture RiskKutay1234No ratings yet
- Evaluation of NK Cells in HCV Patients on HemodialysisDocument13 pagesEvaluation of NK Cells in HCV Patients on HemodialysisMaged SaadNo ratings yet
- Effect of Bacterial Stimulants On Release of Reactive Oxygen Metabolites From Peripheral Blood Neutrophils in PeriodontitisDocument5 pagesEffect of Bacterial Stimulants On Release of Reactive Oxygen Metabolites From Peripheral Blood Neutrophils in PeriodontitisHanny Friska YudistyawanNo ratings yet
- Impact of Anticoagulants on Zinc Level AssessmentDocument5 pagesImpact of Anticoagulants on Zinc Level AssessmentAndrea CardenaNo ratings yet
- Original Article: Assessment of A Lupus Nephritis Cohort Over A 30-Year PeriodDocument7 pagesOriginal Article: Assessment of A Lupus Nephritis Cohort Over A 30-Year PerioddhineyNo ratings yet
- Pharmaceutical SciencesDocument6 pagesPharmaceutical SciencesiajpsNo ratings yet
- Plasma Leptin Levels in Rats With PancreatitisDocument6 pagesPlasma Leptin Levels in Rats With PancreatitisAndykaYayanSetiawanNo ratings yet
- Biochemical, Hematological, and Electrocardiographic Changes in Buffaloes Naturally Infected WithDocument6 pagesBiochemical, Hematological, and Electrocardiographic Changes in Buffaloes Naturally Infected WithKamilahNo ratings yet
- Mineral Metabolism, Mortality, and Morbidity in Maintenance HemodialysisDocument11 pagesMineral Metabolism, Mortality, and Morbidity in Maintenance HemodialysisDaniel CruzNo ratings yet
- The Clinical and Immunologic Effects of AcetylcystDocument2 pagesThe Clinical and Immunologic Effects of Acetylcystفرجني موغNo ratings yet
- Pulmonary Tuberculosis and Its Haematological Correlates-1Document8 pagesPulmonary Tuberculosis and Its Haematological Correlates-1mentari_64No ratings yet
- Gen-Tieu XuowngDocument21 pagesGen-Tieu XuowngphungNo ratings yet
- Left Ventricular Hypertrophy Is Associated With Inflammation in Sodium Loaded Subtotal Nephrectomized RatsDocument8 pagesLeft Ventricular Hypertrophy Is Associated With Inflammation in Sodium Loaded Subtotal Nephrectomized RatsLuis Marcas VilaNo ratings yet
- Jurnal BiomolDocument4 pagesJurnal BiomolDewiakyuNo ratings yet
- 2016 JP Itih3Document11 pages2016 JP Itih3ychuang.leoNo ratings yet
- Manuscript 1Document4 pagesManuscript 1maryNo ratings yet
- Accurate UA Measurement in Patients Receiving Rasburicase TherapyDocument4 pagesAccurate UA Measurement in Patients Receiving Rasburicase TherapysaranyaNo ratings yet
- Oral Tori in Chronic Hemodialysis PatientsDocument7 pagesOral Tori in Chronic Hemodialysis PatientsAbdul Rahman AlmishhdanyNo ratings yet
- Scurvy Masquerading as Rheumatic ConditionsDocument6 pagesScurvy Masquerading as Rheumatic ConditionsZach Segmuel MiñanoNo ratings yet
- Selenium Status Factors in Young BritonsDocument9 pagesSelenium Status Factors in Young BritonsAnonymous owgfxCPNo ratings yet
- Letters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDocument1 pageLetters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDarian AngNo ratings yet
- Lipids in Health and Disease: Correlating Corneal Arcus With Atherosclerosis in Familial HypercholesterolemiaDocument9 pagesLipids in Health and Disease: Correlating Corneal Arcus With Atherosclerosis in Familial HypercholesterolemiagekayuuNo ratings yet
- Reticulocyte hemoglobin content testDocument4 pagesReticulocyte hemoglobin content testLoudry ElfaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
- ABOHNCarGde 032714WEBDocument32 pagesABOHNCarGde 032714WEBAngga Agung SaputraNo ratings yet
- Severe Pulmonary Hypertension and Chronic Obstructive Pulmonary DiseaseDocument6 pagesSevere Pulmonary Hypertension and Chronic Obstructive Pulmonary DiseaseAngga Agung SaputraNo ratings yet
- JurnalDocument7 pagesJurnalAngga Agung SaputraNo ratings yet
- Garvey Gaillard Et Al Emergency CT Scan For SeizuresDocument6 pagesGarvey Gaillard Et Al Emergency CT Scan For SeizuresAngga Agung SaputraNo ratings yet
- Garvey Gaillard Et Al Emergency CT Scan For SeizuresDocument6 pagesGarvey Gaillard Et Al Emergency CT Scan For SeizuresAngga Agung SaputraNo ratings yet
- Agronomy BiofortificationDocument489 pagesAgronomy Biofortification1ab4c100% (2)
- Selenium in Poultry Nutrition and Health (VetBooks - Ir) PDFDocument433 pagesSelenium in Poultry Nutrition and Health (VetBooks - Ir) PDFnasih hamadNo ratings yet
- Plagiarism Checker X Originality Report Similarity Found: 22Document32 pagesPlagiarism Checker X Originality Report Similarity Found: 22Utibe Tibz IkpembeNo ratings yet
- 13 18 PDFDocument6 pages13 18 PDFShahzad Ashraf KhanNo ratings yet
- Paper Procesamiento de Barros Anódicos 2009Document13 pagesPaper Procesamiento de Barros Anódicos 2009Nelson PeñaNo ratings yet
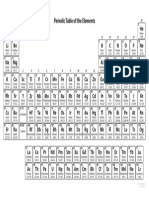
- B & W Periodic TableDocument1 pageB & W Periodic Tableshubham dagaleNo ratings yet
- DENR Accredited LabsDocument16 pagesDENR Accredited LabsThaliaNo ratings yet
- PhysicsDocument16 pagesPhysicsTharaka Dilshan WijekoonNo ratings yet
- Umar, 04 Isyatun RodliyahDocument8 pagesUmar, 04 Isyatun Rodliyahrizky dwi anandaNo ratings yet
- b115 10 Standard Specification For Electrolytic Copper CathodeDocument10 pagesb115 10 Standard Specification For Electrolytic Copper CathodeAlyass EvanNo ratings yet
- Pricelist PDFDocument257 pagesPricelist PDFPrabhakran PerumalNo ratings yet
- Heavy Metal Water Pollution-A Case Study: Recent Research in Science and Technology 2013, 5 (5) : 98-99 ISSN: 2076-5061Document2 pagesHeavy Metal Water Pollution-A Case Study: Recent Research in Science and Technology 2013, 5 (5) : 98-99 ISSN: 2076-5061Zari Sofia LevisteNo ratings yet
- Ijbs 4 89Document8 pagesIjbs 4 89Francisco SalgadoNo ratings yet
- Prabu Et Al. 2017. An Overview On Significance of Fish Nutritionin Aquaculture IndustryDocument8 pagesPrabu Et Al. 2017. An Overview On Significance of Fish Nutritionin Aquaculture IndustryMelissa Espejo CortésNo ratings yet
- Les Articles Et LivresDocument23 pagesLes Articles Et LivresPixel service HosniNo ratings yet
- World Health Organization: Nutrients in Drinking Water (2005)Document196 pagesWorld Health Organization: Nutrients in Drinking Water (2005)Joseph Ford Jr.100% (6)
- AfsDocument35 pagesAfsnora santiNo ratings yet
- TNPCB and PublicDocument187 pagesTNPCB and Publicsaravana_ravichandra100% (1)
- Academic TextDocument3 pagesAcademic Textsonny mark cabangNo ratings yet
- As SuppliesDocument72 pagesAs SuppliesKim HiềnNo ratings yet
- Zenotis Healthcare: TabletsDocument9 pagesZenotis Healthcare: TabletsSudipto PaulNo ratings yet
- Detectors HistoryDocument45 pagesDetectors HistoryENAK9000No ratings yet
- DH 129729Document94 pagesDH 129729sso923No ratings yet
- Optimization FIASDocument10 pagesOptimization FIASDonod DonoNo ratings yet
- Mineral Nutrition of Grazing Goats in Luzon Island, PhilippinesDocument16 pagesMineral Nutrition of Grazing Goats in Luzon Island, PhilippinesJust MeNo ratings yet