You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Principles of Adolescent Substance Use Disorder TreatmentDocument42 pagesPrinciples of Adolescent Substance Use Disorder TreatmentDR DAN PEZZULO100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Cannabis Use DisorderDocument14 pagesCannabis Use Disorderapi-254132646No ratings yet
- Chapter 7-Brief Psychodynamic Therapy: BackgroundDocument54 pagesChapter 7-Brief Psychodynamic Therapy: BackgroundKarenHNo ratings yet
- Marijuana DebateDocument18 pagesMarijuana DebateAldous BasanNo ratings yet
- World Psychiatry - October 2016Document112 pagesWorld Psychiatry - October 2016alfonsougarteNo ratings yet
- Thesis On DrugDocument78 pagesThesis On Drugshumaiyl0% (1)
- Bilirubin T+DDocument2 pagesBilirubin T+DMunawwar AwaNo ratings yet
- ClassificationDocument6 pagesClassificationMunawwar AwaNo ratings yet
- Clinical Evaluation and Radiografic JournalDocument2 pagesClinical Evaluation and Radiografic JournalMunawwar AwaNo ratings yet
- Hari/Tanggal Kegiatan Pukul: Absensi Dokter Muda Bagian Orthopedi Dan TraumatologiDocument15 pagesHari/Tanggal Kegiatan Pukul: Absensi Dokter Muda Bagian Orthopedi Dan TraumatologiMunawwar AwaNo ratings yet
- Jadwal Coass SarafDocument3 pagesJadwal Coass SarafMunawwar AwaNo ratings yet
- Scanned by CamscannerDocument19 pagesScanned by CamscannerMunawwar AwaNo ratings yet
- Endometrial Cancer: BY: Muhammad Munawwar Mohamed Aidil Syahir Wan Salahuddin Ahmad JairullahDocument16 pagesEndometrial Cancer: BY: Muhammad Munawwar Mohamed Aidil Syahir Wan Salahuddin Ahmad JairullahMunawwar AwaNo ratings yet
- Marijuana Intoxication - MedlinePlus Medical EncyclopediaDocument2 pagesMarijuana Intoxication - MedlinePlus Medical EncyclopediaMunawwar AwaNo ratings yet
- SCABIES: A Skin Disease Caused by Sarcoptes ScabieiDocument21 pagesSCABIES: A Skin Disease Caused by Sarcoptes ScabieiMunawwar AwaNo ratings yet
- Marijuana Intoxication - MedlinePlus Medical EncyclopediaDocument2 pagesMarijuana Intoxication - MedlinePlus Medical EncyclopediaMunawwar AwaNo ratings yet
- WHO Recommendation of Antenatal Care For A Positive PDFDocument172 pagesWHO Recommendation of Antenatal Care For A Positive PDFFy DaisyNo ratings yet
- ClassificationDocument6 pagesClassificationMunawwar AwaNo ratings yet
- Chronic SinusitisDocument19 pagesChronic SinusitisMunawwar AwaNo ratings yet
- Cannabinoid Poisoning Treatment & ManagementDocument3 pagesCannabinoid Poisoning Treatment & ManagementMunawwar AwaNo ratings yet
- Chronic SinusitisDocument19 pagesChronic SinusitisMunawwar AwaNo ratings yet
- Fifax - Guddy Files - Fifax.net Fifa14 FIFA14MW 1.7.1. ReadmeDocument14 pagesFifax - Guddy Files - Fifax.net Fifa14 FIFA14MW 1.7.1. ReadmeMunawwar AwaNo ratings yet
- Clinical Evaluation and Radiografic JournalDocument2 pagesClinical Evaluation and Radiografic JournalMunawwar AwaNo ratings yet
- SCABIES: A Skin Disease Caused by Sarcoptes ScabieiDocument21 pagesSCABIES: A Skin Disease Caused by Sarcoptes ScabieiMunawwar AwaNo ratings yet
- Kidney DSDCVASDFStonesDocument4 pagesKidney DSDCVASDFStonesMunawwar AwaNo ratings yet
- Fisiologi Bicara PDFDocument18 pagesFisiologi Bicara PDFMunawwar AwaNo ratings yet
- Nro NotessafdaadDocument199 pagesNro NotessafdaadMunawwar AwaNo ratings yet
- Fifax - Guddy Files - Fifax.net Fifa14 FIFA14MW 1.7.1. ReadmeDocument14 pagesFifax - Guddy Files - Fifax.net Fifa14 FIFA14MW 1.7.1. ReadmeMunawwar AwaNo ratings yet
- Nielsen Et Al-2019-Cochrane Database of Systematic ReviewsDocument4 pagesNielsen Et Al-2019-Cochrane Database of Systematic ReviewsRobbie ShawNo ratings yet
- Legalization of Marijuana For Medical Use in The PhilippinesDocument5 pagesLegalization of Marijuana For Medical Use in The PhilippinesRey Emerson EscuetaNo ratings yet
- Cannabis Related Disorders EditedDocument46 pagesCannabis Related Disorders EditedPriyanka KoundinyaNo ratings yet
- Substance-Related and Addictive Disorders (Presentation)Document219 pagesSubstance-Related and Addictive Disorders (Presentation)Ryan Wong [Aizen]No ratings yet
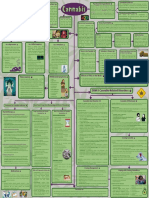
- Cannabis Concept MapDocument2 pagesCannabis Concept MapAminath Maana Ibrahim ShakeeNo ratings yet
- Cannabis Use: Epidemiology, Pharmacology, Comorbidities, and Adverse Effects - UpToDateDocument46 pagesCannabis Use: Epidemiology, Pharmacology, Comorbidities, and Adverse Effects - UpToDateHossdana JimenezNo ratings yet
- G.2 Cannabis Use and Misuse PPT 2019Document50 pagesG.2 Cannabis Use and Misuse PPT 2019Echipa SiposNo ratings yet
- Alcohol, Smoking and Substance Involvement Screening Test (Assist) Linked Brief Intervention (Bi)Document47 pagesAlcohol, Smoking and Substance Involvement Screening Test (Assist) Linked Brief Intervention (Bi)Topz VillarealNo ratings yet
- Review: Kat Petrilli, Shelan Ofori, Lindsey Hines, Gemma Taylor, Sally Adams, Tom P FreemanDocument15 pagesReview: Kat Petrilli, Shelan Ofori, Lindsey Hines, Gemma Taylor, Sally Adams, Tom P FreemansilviaNo ratings yet
- Legalizing Medical and Recreational MarijuanaDocument7 pagesLegalizing Medical and Recreational MarijuanaMwangih LilianNo ratings yet
- Marijuana Abuse by University Students in The USDocument12 pagesMarijuana Abuse by University Students in The USDan Ochieng Jr.No ratings yet
- The Current State of Pharmacological Treatments For Cannabis Use Disorder and WithdrawalDocument22 pagesThe Current State of Pharmacological Treatments For Cannabis Use Disorder and Withdrawalyeremias setyawanNo ratings yet
- RTA AND SUBSTANCE USE DISORDERDocument34 pagesRTA AND SUBSTANCE USE DISORDERAkampurira IanNo ratings yet
- Prevalence and Correlates of Alcohol and Cannabis Use Disorders in the USDocument8 pagesPrevalence and Correlates of Alcohol and Cannabis Use Disorders in the USFadil MuhammadNo ratings yet
- Marijuana Legalization Impact Assessment 7-13-18Document75 pagesMarijuana Legalization Impact Assessment 7-13-18Nick ReismanNo ratings yet
- Sevrage CannabisDocument29 pagesSevrage CannabismihaelaNo ratings yet
- Granny Storm Crow's List Jan 2014 ConditionsDocument750 pagesGranny Storm Crow's List Jan 2014 ConditionsElectroPig Von FökkenGrüüvenNo ratings yet
- Cannabis Use and Cannabis Use DisorderDocument24 pagesCannabis Use and Cannabis Use DisorderHector AngelNo ratings yet
- Psychiatric Disorders and Marijuana UseDocument50 pagesPsychiatric Disorders and Marijuana UseNational Press FoundationNo ratings yet
- Long Essay On Marijuana Essay 500 Words in EnglishDocument3 pagesLong Essay On Marijuana Essay 500 Words in EnglishAli AkbarNo ratings yet
- Social Media Exposure and Drug Abuse Among Adolescent Secondary School StudentsDocument17 pagesSocial Media Exposure and Drug Abuse Among Adolescent Secondary School StudentsMosesNo ratings yet
- 10 Guilt Free 1000mg CBD Vape Cartridges TipsikjzmDocument2 pages10 Guilt Free 1000mg CBD Vape Cartridges Tipsikjzmelbowschool56No ratings yet
- ICD-10-CM Mental Behavioral Neurodevelopmental CodesDocument46 pagesICD-10-CM Mental Behavioral Neurodevelopmental CodesZubair Mahmood KamalNo ratings yet
- The Dangers and Consequences of Marijuana Abuse: Demand Reduction SectionDocument31 pagesThe Dangers and Consequences of Marijuana Abuse: Demand Reduction SectionGiancarlo BarbiniNo ratings yet