You might also like
- 108 Imporant Slokas From BG As It IsDocument34 pages108 Imporant Slokas From BG As It IsShridhar ChameNo ratings yet
- Ajay K. Singh MBBS FRCP Nancy Berliner MD Carolyn B. Becker MD Joseph Loscalzo MD PHD - 41 ST Annual İntensive Review of İnt PDFDocument3,817 pagesAjay K. Singh MBBS FRCP Nancy Berliner MD Carolyn B. Becker MD Joseph Loscalzo MD PHD - 41 ST Annual İntensive Review of İnt PDFShridhar Chame0% (1)
- Psychiatry Review PDFDocument488 pagesPsychiatry Review PDFShridhar Chame100% (11)
- Ramayana Story - Picture FormDocument82 pagesRamayana Story - Picture FormBharath Palepu100% (3)
- PSM Dams PDFDocument198 pagesPSM Dams PDFShridhar ChameNo ratings yet
- DOH National Antibiotic Guidelines 2017Document264 pagesDOH National Antibiotic Guidelines 2017Degee O. Gonzales67% (3)
- DOH National Antibiotic Guidelines 2017Document264 pagesDOH National Antibiotic Guidelines 2017Degee O. Gonzales67% (3)
- Mahabharata - Picture FormDocument142 pagesMahabharata - Picture FormRajesh KolliparaNo ratings yet
- AMR Report Web Slide SetDocument24 pagesAMR Report Web Slide SetShridhar ChameNo ratings yet
- Hiv Easc Guidelines PDFDocument102 pagesHiv Easc Guidelines PDFShridhar ChameNo ratings yet
- Drug Resistance in Bacteria Fungi Malaria PDFDocument629 pagesDrug Resistance in Bacteria Fungi Malaria PDFShridhar Chame100% (1)
- Principles of Pharmacology The Pathophysiologic Basis o DrugDocument1,042 pagesPrinciples of Pharmacology The Pathophysiologic Basis o DrugShridhar Chame100% (1)
- Medicine Update (Vol 28) 2018 PDFDocument1,029 pagesMedicine Update (Vol 28) 2018 PDFShridhar Chame100% (10)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NCP Burn Risk InfectionDocument1 pageNCP Burn Risk InfectionBraingie Racho50% (4)
- PSW Immunization MSDocument2 pagesPSW Immunization MSAngelica Mae FrialaNo ratings yet
- Common ColdDocument3 pagesCommon ColdshaliniNo ratings yet
- Coc Exam ModelDocument44 pagesCoc Exam ModelYeshi AbebeNo ratings yet
- WWW Electroherbalism Com Bioelectronics FrequenciesandAnecdotes CAFL HTMDocument20 pagesWWW Electroherbalism Com Bioelectronics FrequenciesandAnecdotes CAFL HTMjackblack2002No ratings yet
- Diagnostic Manual 2007Document157 pagesDiagnostic Manual 2007warder1100% (1)
- EpiDocument3 pagesEpiNiño PaoloNo ratings yet
- EGRA Summary Pre & Post Test ResultsDocument1 pageEGRA Summary Pre & Post Test ResultsJENEVIEVE MERCADERNo ratings yet
- Blood Anatomy and Physiology: Functions, Components, Groups, and TypingDocument28 pagesBlood Anatomy and Physiology: Functions, Components, Groups, and TypingPORTRAIT OF A NURSENo ratings yet
- How I Investigate Basophilia in Daily Practice: Joffrey Feriel - François Depasse - Franck GenevièveDocument9 pagesHow I Investigate Basophilia in Daily Practice: Joffrey Feriel - François Depasse - Franck GenevièveMarina TaveiraNo ratings yet
- Community Acquired PneumoniaDocument9 pagesCommunity Acquired PneumoniaSuzette Rae TateNo ratings yet
- Granulomatous Inflammation 4Document57 pagesGranulomatous Inflammation 4Siti NabilaNo ratings yet
- Blood Type Test ExperimentDocument8 pagesBlood Type Test ExperimentUpz PhaNo ratings yet
- Expel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerDocument8 pagesExpel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerCarl MacCordNo ratings yet
- Ichroma Anti CCP Plus Rev.03Document4 pagesIchroma Anti CCP Plus Rev.03Laboratorio Medic BactLabNo ratings yet
- Complications of Suppurative Otitis MediaDocument21 pagesComplications of Suppurative Otitis MediaSalsabila Al-BasheerNo ratings yet
- IMMUNOPROPHYLAXISDocument30 pagesIMMUNOPROPHYLAXISAli TARARNo ratings yet
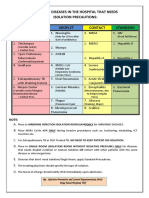
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- Collection, Handling and Labeling of Specimen ProtocolDocument2 pagesCollection, Handling and Labeling of Specimen ProtocolMEDLAB WOODLANDSNo ratings yet
- MCS +: Multicomponent Collection SystemDocument18 pagesMCS +: Multicomponent Collection SystemRamiro LozaNo ratings yet
- AAHA Canine Vaccination GuidelinesDocument23 pagesAAHA Canine Vaccination GuidelinesRaniah DahlanNo ratings yet
- MMI4804 Quiz 5Document16 pagesMMI4804 Quiz 5Ham Mad0% (1)
- Hav Igm CTKDocument2 pagesHav Igm CTKGu AleXanderNo ratings yet
- Chicken Pox PresentationDocument14 pagesChicken Pox Presentationnur syafiqah kamaruzaman100% (3)
- What Is PneumoniaDocument16 pagesWhat Is PneumoniasakuraleeshaoranNo ratings yet
- Kit InsertDocument8 pagesKit InsertMuhammad HamzarNo ratings yet
- FILIRIASISDocument25 pagesFILIRIASISJoy Gao-ayNo ratings yet
- Swapan Kumar Nath Sanjay G Revankar Problem-Based PDFDocument1,163 pagesSwapan Kumar Nath Sanjay G Revankar Problem-Based PDFRestu100% (1)
- Vaccination in PregnancyDocument7 pagesVaccination in PregnancyNoraNo ratings yet
- Microbiology and ParasitologyDocument5 pagesMicrobiology and ParasitologyChester Riogelon100% (2)