You might also like
- Community Health Nursing Practice Questions With RationalesDocument15 pagesCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
- Community Health Nursing Practice Questions With RationalesDocument15 pagesCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
- Drug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument1 pageDrug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesSheana TmplNo ratings yet
- Drug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesDocument1 pageDrug Name Action Indication Contraindication Side Effects Nursing ResponsibilitiesSheana TmplNo ratings yet
- Common Surgical Procedure1Document4 pagesCommon Surgical Procedure1Sheana TmplNo ratings yet
- Nursing TheoriesDocument2 pagesNursing TheoriesSheana TmplNo ratings yet
- Performance Improvement ToolsDocument5 pagesPerformance Improvement ToolsSheana TmplNo ratings yet
- DSA worksheet guides quality improvement cyclesDocument7 pagesDSA worksheet guides quality improvement cyclesSheana TmplNo ratings yet
- Pareto ChartDocument1 pagePareto ChartSheana TmplNo ratings yet
- Pareto ChartDocument1 pagePareto ChartSheana TmplNo ratings yet
- GYNECOLOGICALNURSINGDocument4 pagesGYNECOLOGICALNURSINGSheana TmplNo ratings yet
- Elective II ReviewerDocument4 pagesElective II ReviewerSheana TmplNo ratings yet
- MS 1 PERIOPERATIVE NURSING ROLES AND RESPONSIBILITIESDocument41 pagesMS 1 PERIOPERATIVE NURSING ROLES AND RESPONSIBILITIESSheana TmplNo ratings yet
- ManualDocument9 pagesManualSheana TmplNo ratings yet
- DSA worksheet guides quality improvement cyclesDocument7 pagesDSA worksheet guides quality improvement cyclesSheana TmplNo ratings yet
- Review Eeee ErDocument8 pagesReview Eeee ErSheana TmplNo ratings yet
- NCPDocument3 pagesNCPSheana TmplNo ratings yet
- ANP Heart Anatomy & PhysiologyDocument3 pagesANP Heart Anatomy & PhysiologySheana Tmpl100% (1)
- Nursing HistoryDocument2 pagesNursing HistorySheana TmplNo ratings yet
- Elective IIDocument13 pagesElective IISheana TmplNo ratings yet
- Pathophysiology of Coronary Artery Disease and Myocardial InfarctionDocument2 pagesPathophysiology of Coronary Artery Disease and Myocardial InfarctionSheana TmplNo ratings yet
- Group QuestionsDocument7 pagesGroup QuestionsSheana TmplNo ratings yet
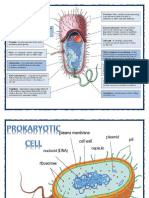
- Prokaryotic CellDocument2 pagesProkaryotic CellSheana TmplNo ratings yet
- Choledocholithias PathophysiologyDocument2 pagesCholedocholithias PathophysiologySheana Tmpl100% (2)
- ObjectivesDocument2 pagesObjectivesSheana TmplNo ratings yet
- Choledocholithias PathophysiologyDocument2 pagesCholedocholithias PathophysiologySheana Tmpl100% (2)
- Walang LamanDocument1 pageWalang LamanSheana TmplNo ratings yet
- First ENCD Youth RallyDocument1 pageFirst ENCD Youth RallySheana TmplNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Afib Simplified Guidelines Treatment Chart UCM - 324032 PDFDocument1 pageAfib Simplified Guidelines Treatment Chart UCM - 324032 PDFLakshay TyagiNo ratings yet
- 12 CR Use of Tenecteplase For PDFDocument4 pages12 CR Use of Tenecteplase For PDFsameeNo ratings yet
- Bor Kavcic: Electrodynamics of Human HeartDocument14 pagesBor Kavcic: Electrodynamics of Human HearttohunabohunNo ratings yet
- Understanding Hepatitis C Discharge InstructionsDocument24 pagesUnderstanding Hepatitis C Discharge InstructionsKatherine Joy ApquisNo ratings yet
- Hahnemannian Gleanings 1979 Vol. 46 Q2Document89 pagesHahnemannian Gleanings 1979 Vol. 46 Q2kolanNo ratings yet
- UWorld Critical CareDocument14 pagesUWorld Critical CareJohnasse Sebastian NavalNo ratings yet
- Anatomy of The Ventricular Septal Defect in Congenital Heart DefectDocument8 pagesAnatomy of The Ventricular Septal Defect in Congenital Heart DefectFajar YuniftiadiNo ratings yet
- Pharmacology of Antiarrhythmic DrugsDocument51 pagesPharmacology of Antiarrhythmic DrugsselflessdoctorNo ratings yet
- NURSING PHARMACOLOGY TIPSDocument19 pagesNURSING PHARMACOLOGY TIPSmaniz442100% (2)
- The 10 Most Common Emergency DrugsDocument28 pagesThe 10 Most Common Emergency DrugsKrishna BalsarzaNo ratings yet
- Chain of Survival: Adult and Pediatric Out of Hospital Cardiac ArrestDocument10 pagesChain of Survival: Adult and Pediatric Out of Hospital Cardiac ArrestJapeth John M. FloresNo ratings yet
- Clinical Worksheet Mary RichardsDocument3 pagesClinical Worksheet Mary RichardsJasmyn RoseNo ratings yet
- 9700 s10 QP 13Document20 pages9700 s10 QP 13Mohamed Abd El HadyNo ratings yet
- May 2021 Question Paper 1BDocument32 pagesMay 2021 Question Paper 1BMeenakshie Chaudrie100% (1)
- Journal Entry 3 Center For Discovery With Theresa CarmichaelDocument9 pagesJournal Entry 3 Center For Discovery With Theresa Carmichaelapi-489592025No ratings yet
- BSM-3000 Lo BR enDocument12 pagesBSM-3000 Lo BR enkizen_5No ratings yet
- 24 de AgostoDocument7 pages24 de Agostoapi-626131140No ratings yet
- P1 RleDocument34 pagesP1 RleMary Jean GicaNo ratings yet
- Digitized Library Book ReproductionDocument575 pagesDigitized Library Book ReproductionMorgan Cabrera0% (1)
- Tee Protocol Bse UkDocument17 pagesTee Protocol Bse UkNavojit ChowdhuryNo ratings yet
- Drug Study NifedipineDocument3 pagesDrug Study NifedipineJanzelvine Lee MontenegroNo ratings yet
- Anatomy MC Question CH 17-22Document4 pagesAnatomy MC Question CH 17-22lmaoheartsNo ratings yet
- Flossing For A Healthier Heart: Date NameDocument4 pagesFlossing For A Healthier Heart: Date Nameadrian jimenezNo ratings yet
- MLT Revised Curriculum (U) 19-12-2019 (Final Version)Document86 pagesMLT Revised Curriculum (U) 19-12-2019 (Final Version)Fawad SawabiNo ratings yet
- PATHOLOGY LE3-mergedDocument18 pagesPATHOLOGY LE3-mergedNdor BariboloNo ratings yet
- The Stabilization of Plaques Using Darapladib (Solid) - Timi 52 Trial: Primary ResultsDocument23 pagesThe Stabilization of Plaques Using Darapladib (Solid) - Timi 52 Trial: Primary ResultsAnnisa Dwi AndrianiNo ratings yet
- Sizing An Aortic Valve For Intervention What Is Important How Does TEE Stack Up - Sniecinski PDFDocument4 pagesSizing An Aortic Valve For Intervention What Is Important How Does TEE Stack Up - Sniecinski PDFduncanmfrNo ratings yet
- Pathophysiology and Etiology of Edema - IDocument9 pagesPathophysiology and Etiology of Edema - IBrandy MaddoxNo ratings yet
- Case Study 29Document2 pagesCase Study 29Edna MooreNo ratings yet
- MODULE 1.1 and 1.2 SOFTDocument5 pagesMODULE 1.1 and 1.2 SOFTJason SebastianNo ratings yet