You might also like
- Cefotaxime Drug Class, Uses, Side EffectsDocument3 pagesCefotaxime Drug Class, Uses, Side EffectsKristi WrayNo ratings yet
- Case Study NCP ActualDocument3 pagesCase Study NCP Actualdhamy florNo ratings yet
- Normal Spontaneous DeliveryDocument11 pagesNormal Spontaneous DeliveryAyah GarciaNo ratings yet
- NCP - ERDocument5 pagesNCP - ERAnnelore ArcayNo ratings yet
- Burn - Concept MapDocument1 pageBurn - Concept MapAaron RafaelNo ratings yet
- PrioritizationDocument1 pagePrioritizationJLAZRONo ratings yet
- DS OfloxacinDocument2 pagesDS OfloxacinjessicamaysNo ratings yet
- DP Discharge Plan@@@@@@@@Document6 pagesDP Discharge Plan@@@@@@@@Maemae SumalinogNo ratings yet
- Nursing Care Plan for Clear Airway GoalDocument9 pagesNursing Care Plan for Clear Airway GoalSkyerexNo ratings yet
- CetirizineDocument1 pageCetirizineGabby Robles PajeNo ratings yet
- CefuroximeDocument11 pagesCefuroximeAlmira Ballesteros CestonaNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument2 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- Drug Study Pedia WardDocument2 pagesDrug Study Pedia WardCayanne ChuaNo ratings yet
- F&E Drug StudyDocument2 pagesF&E Drug Studychelle_asenjoNo ratings yet
- DRUG-STUDY - BALLON, Karlo CDocument6 pagesDRUG-STUDY - BALLON, Karlo CMelinda Cariño BallonNo ratings yet
- Discharge PlanDocument3 pagesDischarge PlanDranlie LagdamenNo ratings yet
- Ertapenem (Invanz)Document1 pageErtapenem (Invanz)Adrianne BazoNo ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document1 pageDysfunctional Uterine Bleeding (DUB)Bheru LalNo ratings yet
- Pneumonia Drug StudyDocument3 pagesPneumonia Drug Studyatienza02No ratings yet
- Medication ThalassemiaDocument3 pagesMedication ThalassemiaDivya ToppoNo ratings yet
- Nahco3 Vancomycin AmlodipineDocument3 pagesNahco3 Vancomycin AmlodipineShan Dave TupasNo ratings yet
- Common Side Effects of Oxytocin Include:: CNS: Maternal: COMADocument3 pagesCommon Side Effects of Oxytocin Include:: CNS: Maternal: COMAann camposNo ratings yet
- Nursing Assessment, Planning, Intervention and Evaluation for Community-Acquired Pneumonia (CAPDocument6 pagesNursing Assessment, Planning, Intervention and Evaluation for Community-Acquired Pneumonia (CAPIngrid Eunice ConcordiaNo ratings yet
- Biperiden Generic and Brand Names, Uses, Side EffectsDocument1 pageBiperiden Generic and Brand Names, Uses, Side EffectsMFQ.RN100% (2)
- Nursing Care PlanDocument3 pagesNursing Care PlanAnnahNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanVillanueva NiñaNo ratings yet
- Azithromycin Nursing ConsiderationsDocument2 pagesAzithromycin Nursing ConsiderationsKristine YoungNo ratings yet
- Drug Study Case PresentationDocument5 pagesDrug Study Case PresentationRobert MedinaNo ratings yet
- Discharge Plan With Other ReferncesDocument3 pagesDischarge Plan With Other ReferncesApril Joy PrestoNo ratings yet
- NCP Ineffective Airway ClearanceDocument1 pageNCP Ineffective Airway Clearancejae_007No ratings yet
- 3011-1 - NCP & Drug Study - AMCDocument5 pages3011-1 - NCP & Drug Study - AMCAngie MandeoyaNo ratings yet
- Virtual Clinical Duty Daily RequirementsDocument7 pagesVirtual Clinical Duty Daily RequirementsEdgie FabreNo ratings yet
- Nursing Care Plan for a Patient with Multiple Bruises and Difficulty BreathingDocument3 pagesNursing Care Plan for a Patient with Multiple Bruises and Difficulty BreathingLeogalvez BedanoNo ratings yet
- Pedia Care Study - Appendix B - Drug StudyDocument8 pagesPedia Care Study - Appendix B - Drug Studyryan100% (1)
- Nifedipine Drug StudyDocument2 pagesNifedipine Drug StudyMary Shane MoraldeNo ratings yet
- Health Teaching Plan DyspneaDocument3 pagesHealth Teaching Plan DyspneaMae JavierNo ratings yet
- Cefipime HCL (AXERA)Document2 pagesCefipime HCL (AXERA)Kristine YoungNo ratings yet
- Tpo Eo Poa LFDDocument4 pagesTpo Eo Poa LFDEzra Miguel DarundayNo ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument3 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- Nursing Care Plan for Fever, Hyperthermia, High TemperatureDocument2 pagesNursing Care Plan for Fever, Hyperthermia, High TemperatureVanessa AbboudNo ratings yet
- Criteria Computation Score JustificationDocument5 pagesCriteria Computation Score JustificationCharm JavierNo ratings yet
- Tpo Ward BMDocument3 pagesTpo Ward BMAhl A PurujiNo ratings yet
- NCP Knowledge Deficient FPDocument2 pagesNCP Knowledge Deficient FPDayanaj OngNo ratings yet
- Essential care universally available at affordable cost defined as primary health careDocument11 pagesEssential care universally available at affordable cost defined as primary health careAngelina Janiya NicoleNo ratings yet
- Drug StudyDocument4 pagesDrug StudyPam RomeroNo ratings yet
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document3 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Duchess Juliane Jose MirambelNo ratings yet
- Case Study Peralta (Drug N NCP)Document10 pagesCase Study Peralta (Drug N NCP)Trisha Cruise100% (1)
- ER Platinum Drug GuideDocument28 pagesER Platinum Drug Guideiscariot02No ratings yet
- Assessing and Treating Post-Operative HypothermiaDocument2 pagesAssessing and Treating Post-Operative HypothermiaJayrelle D. SafranNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Hepatitis A PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis A PDFswapnilazarusNo ratings yet
- Concept MapDocument1 pageConcept MapNicole Ivy GorimoNo ratings yet
- Methyldopa nursing management for hypertensionDocument4 pagesMethyldopa nursing management for hypertensionRico Mae ValenciaNo ratings yet
- Steps RationaleDocument3 pagesSteps RationaleKangMunching PotatoGamingNo ratings yet
- Drug AnalysisDocument8 pagesDrug AnalysisJonie Vince SañosaNo ratings yet
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- Kocher (Ochsner) .: (Kelly Curve) - Use To Clamp Larger Tissues or VesselsDocument5 pagesKocher (Ochsner) .: (Kelly Curve) - Use To Clamp Larger Tissues or VesselsKevin AliasasNo ratings yet
- NafarinDocument2 pagesNafarinianecunar100% (2)
- Difficulty Breathing Intervention and EvaluationDocument1 pageDifficulty Breathing Intervention and EvaluationJamaica Leslie NovenoNo ratings yet
- Ceftriaxone PDFDocument3 pagesCeftriaxone PDFLauren JalandoniNo ratings yet
- Meropenem Dosage, Interactions and Nursing ConsiderationsDocument2 pagesMeropenem Dosage, Interactions and Nursing ConsiderationsJewel BrondaNo ratings yet
- Isfahan Dwi Putra 22010111110146 Lap - Kti BAB8Document28 pagesIsfahan Dwi Putra 22010111110146 Lap - Kti BAB8MargotNo ratings yet
- 050547s068,050596s037lbl PDFDocument18 pages050547s068,050596s037lbl PDFMargotNo ratings yet
- Uji Aktivitas Antioksidan Ekstrak Belimbing Wuluh - Averrhoa Bilimbi, L. - Terhadap 1,1-Diphenyl-2-Picrylhidrazyl - DPPHDocument9 pagesUji Aktivitas Antioksidan Ekstrak Belimbing Wuluh - Averrhoa Bilimbi, L. - Terhadap 1,1-Diphenyl-2-Picrylhidrazyl - DPPHArifin I. OputuNo ratings yet
- 1 SMDocument8 pages1 SMMargotNo ratings yet
- 6 11 1 SM PDFDocument4 pages6 11 1 SM PDFMargotNo ratings yet
- 1 SMDocument9 pages1 SMMargotNo ratings yet
- 1 SMDocument8 pages1 SMMargotNo ratings yet
- Keywords: Bromelain, Cyclooxigenase, ProstaglandinDocument7 pagesKeywords: Bromelain, Cyclooxigenase, ProstaglandinMargotNo ratings yet
- Properties and Therapeutic Application of Bromelain: A ReviewDocument8 pagesProperties and Therapeutic Application of Bromelain: A ReviewMargotNo ratings yet
- 268 607 1 PB PDFDocument7 pages268 607 1 PB PDFMargotNo ratings yet
- Diabetic Nephropathy ReferencesDocument11 pagesDiabetic Nephropathy ReferencesMargotNo ratings yet
- Diabetic Nephropathy ReferencesDocument11 pagesDiabetic Nephropathy ReferencesMargotNo ratings yet
- Diabetic Nephropathy ReferencesDocument11 pagesDiabetic Nephropathy ReferencesMargotNo ratings yet
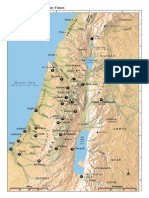
- Israel Bible MapDocument1 pageIsrael Bible MapMoses_JakkalaNo ratings yet
- Maurice Strong by Henry LambDocument9 pagesMaurice Strong by Henry LambHal ShurtleffNo ratings yet
- 25 Virtues Explained with Real Life SituationsDocument5 pages25 Virtues Explained with Real Life Situationsleslie vine deloso100% (2)
- Teacher swap agreement for family reasonsDocument4 pagesTeacher swap agreement for family reasonsKimber LeeNo ratings yet
- McKesson Point of Use Supply - FINALDocument9 pagesMcKesson Point of Use Supply - FINALAbduRahman MuhammedNo ratings yet
- Healthy Kitchen Shortcuts: Printable PackDocument12 pagesHealthy Kitchen Shortcuts: Printable PackAndre3893No ratings yet
- Module 3 - Risk Based Inspection (RBI) Based On API and ASMEDocument4 pagesModule 3 - Risk Based Inspection (RBI) Based On API and ASMEAgustin A.No ratings yet
- HM5 - ScriptDocument4 pagesHM5 - ScriptCamilleTizonNo ratings yet
- Evolution of The Indian Legal System 2Document7 pagesEvolution of The Indian Legal System 2Akhil YarramreddyNo ratings yet
- Torts and DamagesDocument63 pagesTorts and DamagesStevensonYuNo ratings yet
- Presentations - Benefits of WalkingDocument1 pagePresentations - Benefits of WalkingEde Mehta WardhanaNo ratings yet
- SPACES Nepal - Green Schools Building The FutureDocument3 pagesSPACES Nepal - Green Schools Building The FutureBimal ThapaNo ratings yet
- Mariam Kairuz property dispute caseDocument7 pagesMariam Kairuz property dispute caseReginald Matt Aquino SantiagoNo ratings yet
- Managing Director Insurance M&A Advisory in Hong Kong Resume John SpenceDocument3 pagesManaging Director Insurance M&A Advisory in Hong Kong Resume John SpenceJohnSpence2No ratings yet
- Adjusted School Reading Program of Buneg EsDocument7 pagesAdjusted School Reading Program of Buneg EsGener Taña AntonioNo ratings yet
- M8 UTS A. Sexual SelfDocument10 pagesM8 UTS A. Sexual SelfAnon UnoNo ratings yet
- Trinity R&P Keyboards Syllabus From 2018Document54 pagesTrinity R&P Keyboards Syllabus From 2018VickyNo ratings yet
- Pot PPTDocument35 pagesPot PPTRandom PersonNo ratings yet
- Monohybrid Cross WorksheetDocument2 pagesMonohybrid Cross WorksheetLovie Alfonso0% (1)
- SEIPIDocument20 pagesSEIPIdexterbautistadecember161985No ratings yet
- Bell I Do Final PrintoutDocument38 pagesBell I Do Final PrintoutAthel BellidoNo ratings yet
- Timpuri Verbale Engleza RezumatDocument5 pagesTimpuri Verbale Engleza RezumatBogdan StefanNo ratings yet
- How To Use Google FormsDocument126 pagesHow To Use Google FormsBenedict Bagube100% (1)
- Once in his Orient: Le Corbusier and the intoxication of colourDocument4 pagesOnce in his Orient: Le Corbusier and the intoxication of coloursurajNo ratings yet
- Álvaro García Linera A Marxist Seduced BookDocument47 pagesÁlvaro García Linera A Marxist Seduced BookTomás TorresNo ratings yet
- AmulDocument4 pagesAmulR BNo ratings yet
- Installation, Operation and Maintenance Instructions Stainless Steel, Liquid Ring Vacuum PumpsDocument28 pagesInstallation, Operation and Maintenance Instructions Stainless Steel, Liquid Ring Vacuum PumpspinplataNo ratings yet
- How To Make Wall Moulding Design For Rooms Accent Wall Video TutorialsDocument15 pagesHow To Make Wall Moulding Design For Rooms Accent Wall Video Tutorialsdonaldwhale1151No ratings yet
- Exp Mun Feb-15 (Excel)Document7,510 pagesExp Mun Feb-15 (Excel)Vivek DomadiaNo ratings yet
- Bo de On Thi Hoc Ki 1 Lop 3 Mon Tieng AnhDocument66 pagesBo de On Thi Hoc Ki 1 Lop 3 Mon Tieng AnhHằng DiệuNo ratings yet