You might also like
- Empirical Prescribing Chart GlasgowDocument1 pageEmpirical Prescribing Chart GlasgowHariharan Narendran75% (4)
- Career Guidance For Grade11Document116 pagesCareer Guidance For Grade11Felipe Balinas67% (3)
- The History of Occupational TherapyDocument17 pagesThe History of Occupational TherapyHannah GuintoNo ratings yet
- Disorders of Thought and SpeechDocument50 pagesDisorders of Thought and SpeechTilarupa BhattaraiNo ratings yet
- Sepsis 3Document38 pagesSepsis 3EvanNo ratings yet
- Learn Ejaculatory Control in 4 Easy StepsDocument3 pagesLearn Ejaculatory Control in 4 Easy StepsWilliam PayneNo ratings yet
- Sai Vibrionics Newsletter From The Desk of DR Jit K AggarwalDocument18 pagesSai Vibrionics Newsletter From The Desk of DR Jit K AggarwalSujok Swadesh100% (1)
- Range of MotionDocument17 pagesRange of MotionJim Cariaga100% (2)
- Gagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanDocument20 pagesGagal Napas: Pembimbing Dr. Ngakan Putu Parsama Putra, SPP (K) Presenter Dr. Muli YamanAdlan BinharyantoNo ratings yet
- The Settings Processes Methods and ToolsDocument33 pagesThe Settings Processes Methods and ToolsJhay SeresacNo ratings yet
- CSS Airway Management RickyDocument53 pagesCSS Airway Management RickyArtha PutuNo ratings yet
- III Semester: Specialisation IDocument3 pagesIII Semester: Specialisation IJagat BasumatariNo ratings yet
- Cellular and Molecular Actions of Methylene Blue in The Nervous System - Oz Et Al.Document25 pagesCellular and Molecular Actions of Methylene Blue in The Nervous System - Oz Et Al.estebanNo ratings yet
- Krisis Tiroid: Diagnosis Dan TatalaksanaDocument24 pagesKrisis Tiroid: Diagnosis Dan TatalaksanaEpifani Angelina ChandraNo ratings yet
- Peterson, Severin - A Catalog of The Ways People Grow PDFDocument383 pagesPeterson, Severin - A Catalog of The Ways People Grow PDFvivaldioz100% (2)
- The 10 Min Geriatric AssessmentDocument44 pagesThe 10 Min Geriatric AssessmentAndy F MonroeNo ratings yet
- Management of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesDocument10 pagesManagement of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesArizkamhNo ratings yet
- Deep Vein ThrombosisDocument16 pagesDeep Vein ThrombosisB1 TutorialNo ratings yet
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocument21 pagesMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariNo ratings yet
- Materi Kelainan ParuDocument72 pagesMateri Kelainan ParuDebiNingtyasDwiKusumaWardaniNo ratings yet
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDocument57 pagesCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocument60 pagesTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNo ratings yet
- Tehnik - Tehnik Analgesia Post OperasiDocument32 pagesTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoNo ratings yet
- Manajemen Disritmia Kardiak IntraoperatifDocument53 pagesManajemen Disritmia Kardiak IntraoperatifAbi FaizNo ratings yet
- PVC Stoelting Coex 1Document29 pagesPVC Stoelting Coex 1Rudy SiahaanNo ratings yet
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNo ratings yet
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonNo ratings yet
- Deresuscitation ARDSDocument28 pagesDeresuscitation ARDSSudaryadiNo ratings yet
- THT Bimbel Ukdi Mantap 2015 - NorestrictionDocument227 pagesTHT Bimbel Ukdi Mantap 2015 - NorestrictionpanduNo ratings yet
- MediastinumDocument27 pagesMediastinumAndrei PanaNo ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNo ratings yet
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DNo ratings yet
- Taping OA Genu Dr. SIsca Susantio, Sp. KFRDocument11 pagesTaping OA Genu Dr. SIsca Susantio, Sp. KFRDsk IndryNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
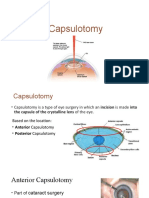
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- PratikPatel - Duodenal AtresiaDocument1 pagePratikPatel - Duodenal AtresiaIkhlasia Amali MahzumNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- AnestesiDocument59 pagesAnestesiJeffrey EkaNo ratings yet
- HDDocument23 pagesHDSardjitoNo ratings yet
- Praseno Hadi - ARDS (Malang 2018)Document25 pagesPraseno Hadi - ARDS (Malang 2018)Rian HutabaratNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Managing Brain Injury AnesthesiaDocument62 pagesManaging Brain Injury AnesthesiaKelvin KelvinNo ratings yet
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Document17 pagesKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNo ratings yet
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- Konas Perdatin 2019Document66 pagesKonas Perdatin 2019Akreditasi RSPC19No ratings yet
- Teknik Foto X Ray EkstremitasDocument14 pagesTeknik Foto X Ray EkstremitasEdiPtkNo ratings yet
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemNo ratings yet
- PPT Referat ADHD - Kevin LukitoDocument22 pagesPPT Referat ADHD - Kevin LukitonoviaNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Hemodynamic Monitoring I ABP CVP AoDocument35 pagesHemodynamic Monitoring I ABP CVP AoNofilia Citra CandraNo ratings yet
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- Deskripsi MurmurDocument3 pagesDeskripsi MurmurLevina Tri RatanaNo ratings yet
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahNo ratings yet
- DRUG ERUPTION GUIDEDocument46 pagesDRUG ERUPTION GUIDESyahDikaNo ratings yet
- Modern View of AsthmaDocument27 pagesModern View of AsthmaraisaNo ratings yet
- Catatan DSTC CourseDocument3 pagesCatatan DSTC CourseHanny FadhilaNo ratings yet
- ROZERPLASTYDocument13 pagesROZERPLASTYSaraya AmajidaNo ratings yet
- Adjuvan Anestesia PresentationDocument53 pagesAdjuvan Anestesia PresentationAdi Chand100% (1)
- Episkleritis N Skleritis EditDocument12 pagesEpiskleritis N Skleritis EditAnonymous HgX3mN1oNo ratings yet
- Malignant Soft Tissue TumorsDocument21 pagesMalignant Soft Tissue TumorsEva GustianiNo ratings yet
- Ca GasterDocument27 pagesCa GastermerryNo ratings yet
- Understanding NystagmusDocument14 pagesUnderstanding NystagmusJefferson CaesarioNo ratings yet
- Difficult AirwayDocument38 pagesDifficult AirwaybrojeemNo ratings yet
- Kuliah Extrapyramidal SyndromeDocument50 pagesKuliah Extrapyramidal SyndromePutri Azka RinandaNo ratings yet
- Burat-Buret Echo Romi Revised PDFDocument2 pagesBurat-Buret Echo Romi Revised PDFAsma.denmiNo ratings yet
- Ear Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniDocument76 pagesEar Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniAldy Bima100% (1)
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaFrom EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaNo ratings yet
- Either Silent or Switched OffDocument67 pagesEither Silent or Switched OffPankaj Kumar Singh100% (1)
- Costy Pandjaitan, SKM.,MARSDocument49 pagesCosty Pandjaitan, SKM.,MARSsilviNo ratings yet
- Care Bundels Stop Infections - DR - RosenthalDocument120 pagesCare Bundels Stop Infections - DR - RosenthalsilviNo ratings yet
- Checklist Safety InjectionDocument1 pageChecklist Safety InjectionsilviNo ratings yet
- Aplikasi Bundels Central Vena LineDocument32 pagesAplikasi Bundels Central Vena LinesilviNo ratings yet
- Guidelines On Hand HygieneDocument270 pagesGuidelines On Hand HygieneDr. Vikram Lotwala100% (1)
- Hildegard PeplauDocument8 pagesHildegard PeplauNeven BuhinNo ratings yet
- 2017medical CertificateDocument3 pages2017medical CertificateJenevieve umayamNo ratings yet
- ActelionDocument124 pagesActelionSilviu CiocianuNo ratings yet
- Peran Akupunktur Medik Pada Kasus NyeriDocument155 pagesPeran Akupunktur Medik Pada Kasus NyeriSilvia HandikaNo ratings yet
- Case Presentation: "Aggression" Module Scenario 2 Group 2Document28 pagesCase Presentation: "Aggression" Module Scenario 2 Group 2Fatimah OthmanNo ratings yet
- Patch AdamDocument15 pagesPatch AdamNabila SyahiraNo ratings yet
- Ooi 150050Document7 pagesOoi 150050MelaNia Elonk ZamroniNo ratings yet
- Open Fractures: DR Jaka Sefta PerdanaDocument75 pagesOpen Fractures: DR Jaka Sefta PerdanaJaka Sefta PerdanaNo ratings yet
- Craniotomy Procedure and Post-Op CareDocument23 pagesCraniotomy Procedure and Post-Op CareUmar FarooqNo ratings yet
- 2013DRAFTMEMSProtocols062713 PDFDocument134 pages2013DRAFTMEMSProtocols062713 PDFMarian Ioan-LucianNo ratings yet
- Day Care For Older People - Greater AucklandDocument17 pagesDay Care For Older People - Greater AucklandnzdocNo ratings yet
- The Intentional Application of Humor With CKD PatientsDocument8 pagesThe Intentional Application of Humor With CKD PatientsKaryn BuxmanNo ratings yet
- Acute Myocardial InfarctionDocument20 pagesAcute Myocardial InfarctionDavid Christian CalmaNo ratings yet
- Pravastatin SodiumDocument3 pagesPravastatin Sodiumapi-3797941No ratings yet
- Thalasemmia, Hemophilia & Blood Cancer at Hamza Foundation Peshawar Field Work Report by Fakhre Alam Mohmand Dept of Social Work University of PeshawarDocument26 pagesThalasemmia, Hemophilia & Blood Cancer at Hamza Foundation Peshawar Field Work Report by Fakhre Alam Mohmand Dept of Social Work University of PeshawarFakhrealamswNo ratings yet
- Minor Tooth Correction With The "Essix System" - A Case ReportDocument2 pagesMinor Tooth Correction With The "Essix System" - A Case Reportdent in dentistNo ratings yet
- Aaron Bonert: Campus: HomeDocument2 pagesAaron Bonert: Campus: Homeapi-239757889No ratings yet
- Treatment of Glioblastoma With Herbal MedicinesDocument14 pagesTreatment of Glioblastoma With Herbal MedicinesGabrielAbarcaNo ratings yet