You might also like
- UntitledDocument1 pageUntitledIcha IchaNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Jurnal PDFDocument14 pagesJurnal PDFIcha IchaNo ratings yet
- Jurnal PDFDocument14 pagesJurnal PDFIcha IchaNo ratings yet
- Irritable Bowel SyndromeDocument28 pagesIrritable Bowel SyndromeNimish ShahNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Pharmacological Aspects: Substance Abuse in Patients With SchizophreniaDocument7 pagesPharmacological Aspects: Substance Abuse in Patients With SchizophreniaKaka kamamNo ratings yet
- Perencanaan SDMDocument13 pagesPerencanaan SDMHafiz Wira PutraNo ratings yet
- Laboratory Calculations Handouts Jones PDFDocument29 pagesLaboratory Calculations Handouts Jones PDFIcha IchaNo ratings yet
- Laboratory Calculations Handouts Jones PDFDocument29 pagesLaboratory Calculations Handouts Jones PDFIcha IchaNo ratings yet
- Irritable Bowel SyndromeDocument28 pagesIrritable Bowel SyndromeNimish ShahNo ratings yet
- DXM Profile: Effects, Risks of Cough Medicine AbuseDocument4 pagesDXM Profile: Effects, Risks of Cough Medicine AbuseIcha IchaNo ratings yet
- Wei 2016Document17 pagesWei 2016Icha IchaNo ratings yet
- Newman Toker 2015Document23 pagesNewman Toker 2015Icha IchaNo ratings yet
- Meningiomas A Clinicopathological StudyDocument10 pagesMeningiomas A Clinicopathological StudyIcha IchaNo ratings yet
- Superior Vena Cava Obstruction - Radiology Reference Article PDFDocument10 pagesSuperior Vena Cava Obstruction - Radiology Reference Article PDFIcha IchaNo ratings yet
- Meningiomas A Clinicopathological Study PDFDocument5 pagesMeningiomas A Clinicopathological Study PDFIcha IchaNo ratings yet
- Tumor IntrakranialDocument14 pagesTumor IntrakranialIcha IchaNo ratings yet
- Superior Vena Cava Obstruction - Radiology Reference Article PDFDocument10 pagesSuperior Vena Cava Obstruction - Radiology Reference Article PDFIcha IchaNo ratings yet
- Fi 208Document10 pagesFi 208Icha IchaNo ratings yet
- Cohrane ReviewDocument55 pagesCohrane ReviewIcha IchaNo ratings yet
- 333 645 1 SMDocument7 pages333 645 1 SMStephanie ThompsonNo ratings yet
- 333 645 1 SMDocument7 pages333 645 1 SMStephanie ThompsonNo ratings yet
- Left Atrial EnlargementDocument14 pagesLeft Atrial EnlargementIcha IchaNo ratings yet
- Jurnal SarafDocument240 pagesJurnal SarafIcha IchaNo ratings yet
- Bls IcgDocument10 pagesBls IcgIcha IchaNo ratings yet
- The Radiology AssistantDocument30 pagesThe Radiology AssistantIcha IchaNo ratings yet
- Bls IcgDocument10 pagesBls IcgIcha IchaNo ratings yet
- Lubchanco Classification - of - Newborns-Boysgirls PDFDocument1 pageLubchanco Classification - of - Newborns-Boysgirls PDFIcha Icha100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Respiratory PhysiologyDocument37 pagesRespiratory PhysiologyGuillermo Sasso Pacheco100% (1)
- Case Study: Pleural Effusion: Union Christian CollegeDocument8 pagesCase Study: Pleural Effusion: Union Christian CollegeJobelle AcenaNo ratings yet
- Functional anatomy of pulmonary system, pulmonary circulation and mechanics of breathingDocument98 pagesFunctional anatomy of pulmonary system, pulmonary circulation and mechanics of breathingdrusmanjamilhcmdNo ratings yet
- Pleural Conditions: Pleurisy (Pleuritis)Document10 pagesPleural Conditions: Pleurisy (Pleuritis)merin sunilNo ratings yet
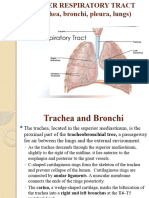
- Trachea and LungsDocument25 pagesTrachea and LungsDr.pallavi kumariNo ratings yet
- Diagnosis and Management of Pleural TransudatesDocument8 pagesDiagnosis and Management of Pleural Transudatesvictor ibarra romeroNo ratings yet
- Lower Resp TractDocument32 pagesLower Resp TractTakshikaNo ratings yet
- ILO Classification For PneumoconiosisDocument51 pagesILO Classification For PneumoconiosisdesichNo ratings yet
- FOM Study Guide: Pleural Cavity, Lung Volumes & EffusionsDocument3 pagesFOM Study Guide: Pleural Cavity, Lung Volumes & EffusionsBernadine Cruz Par100% (1)
- Diagnostic in Pulmonary Emergency and Respiratory Problem 2020 PDFDocument43 pagesDiagnostic in Pulmonary Emergency and Respiratory Problem 2020 PDFIzka P RahmaniaNo ratings yet
- Practise Questions Keith & Moore 5th Edition - Should ReadDocument113 pagesPractise Questions Keith & Moore 5th Edition - Should ReadAmirsalar Eslami83% (6)
- The International System For Reporting Serous Fluid Cytopathology Diagnostic Categories and Clinical ManagementDocument30 pagesThe International System For Reporting Serous Fluid Cytopathology Diagnostic Categories and Clinical ManagementPaulo E M SouzaNo ratings yet
- Transudate or ExudateDocument6 pagesTransudate or ExudateDattatreyaNo ratings yet
- Diagnosing Pleural EffusionsDocument49 pagesDiagnosing Pleural Effusionsdale 99No ratings yet
- Chest CT Signs in Pulmonary Disease PDFDocument19 pagesChest CT Signs in Pulmonary Disease PDFpvs5155No ratings yet
- IM-CAP Concept MapDocument1 pageIM-CAP Concept MapTrisNo ratings yet
- 2 ItemDocument9 pages2 ItemDaniberg RimenisNo ratings yet
- Pneumothorax Case FileDocument2 pagesPneumothorax Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Thoracic & Abdominal Wall BlocksDocument57 pagesThoracic & Abdominal Wall Blocksvignoth23112000No ratings yet
- Empyema: By-Komal JaiswalDocument29 pagesEmpyema: By-Komal JaiswalOlga GoryachevaNo ratings yet
- Case Presentation On Myocardial Infarction LalanDocument8 pagesCase Presentation On Myocardial Infarction Lalananimesh pandaNo ratings yet
- W Masi AssignmentDocument9 pagesW Masi AssignmentBinoyNo ratings yet
- Case Study On PneumoniaDocument31 pagesCase Study On PneumoniaLarah Mae Andog85% (20)
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- Chapter 25 Egans 10th Edition Workbook Answer KeyDocument10 pagesChapter 25 Egans 10th Edition Workbook Answer KeyStevenPaulDacles100% (1)
- Shaukat Khanum Memorial Cancer Hospital & Research CentreDocument2 pagesShaukat Khanum Memorial Cancer Hospital & Research CentreMa BeNo ratings yet
- Stool Analysis and Other Body Fluid AnalysisDocument51 pagesStool Analysis and Other Body Fluid AnalysisPutri Senna Rahayu100% (2)
- Pemicu 2 Blok KGD Jovian LutfiDocument77 pagesPemicu 2 Blok KGD Jovian LutfiJovian LutfiNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaapalahartinamaNo ratings yet