You might also like
- Conners - Material - 2Document1 pageConners - Material - 2saraNo ratings yet
- Kim Gilbert 2018 PDFDocument25 pagesKim Gilbert 2018 PDFKim Gilbert50% (2)
- Health Insurance Application FormDocument2 pagesHealth Insurance Application FormFrenzy Taher100% (1)
- Philippine Health Insurance Corporation: Republic of The PhilippinesDocument2 pagesPhilippine Health Insurance Corporation: Republic of The Philippinesangga2681No ratings yet
- Family Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsDocument2 pagesFamily Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsnomiabbasiNo ratings yet
- CRP g6 NF Cyborg AthletesDocument1 pageCRP g6 NF Cyborg Athletesapi-462707193No ratings yet
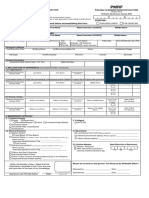
- PMRFDocument2 pagesPMRFKrizel Joy Serrano90% (10)
- Life Insurance Beneficiary Designation Form - GeneraliDocument2 pagesLife Insurance Beneficiary Designation Form - Generalijohn gerald reynoNo ratings yet
- Required, They Should Be Sent To Our National Document Center at P.O. Box 258806, Oklahoma City, OK 73125-8806Document3 pagesRequired, They Should Be Sent To Our National Document Center at P.O. Box 258806, Oklahoma City, OK 73125-8806Theo HerspergerNo ratings yet
- Hitachi Solutions - ETIQA - Application FormDocument1 pageHitachi Solutions - ETIQA - Application FormBernard CasimiroNo ratings yet
- Child Care Application and Authorization Form for First Responders and Healthcare WorkersDocument4 pagesChild Care Application and Authorization Form for First Responders and Healthcare WorkersRaistlin Julian GreenwaltNo ratings yet
- SunLife Group Benefits EnrollmentDocument4 pagesSunLife Group Benefits Enrollmentsanjaysingh829356No ratings yet
- Instructions for the Statement of Health FormDocument5 pagesInstructions for the Statement of Health FormRajendra PilludaNo ratings yet
- Application For Individual Insurance FormDocument2 pagesApplication For Individual Insurance FormShenna RojasNo ratings yet
- Please Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeDocument2 pagesPlease Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeArnelyn Garnace AgraNo ratings yet
- Group Insurance ApplicationDocument1 pageGroup Insurance Applicationジョン ジーNo ratings yet
- Medical FormDocument2 pagesMedical Formantay.halder19No ratings yet
- AIA Singapore Health Declaration FormDocument4 pagesAIA Singapore Health Declaration FormkotisanampudiNo ratings yet
- Medical Benefits For Qualified Dependents Enrolment/Cancelation FormDocument1 pageMedical Benefits For Qualified Dependents Enrolment/Cancelation FormAnne MartinezNo ratings yet
- Health insurance enrollment formDocument1 pageHealth insurance enrollment formPrashanth PrakashNo ratings yet
- Philippines Health Insurance FormDocument2 pagesPhilippines Health Insurance FormDBVS GRAY MORTERANo ratings yet
- Please Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeDocument2 pagesPlease Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeMosses BryanNo ratings yet
- Sunlife Grepa Application FormDocument2 pagesSunlife Grepa Application Formkathreentracy0% (1)
- A Guide For Successfully Completing The Group Insurance Evidence of Insurability FormDocument9 pagesA Guide For Successfully Completing The Group Insurance Evidence of Insurability FormVaishakNo ratings yet
- ESAP FormsDocument17 pagesESAP FormsKa PuringNo ratings yet
- Authorization To Release Medical CertificateDocument1 pageAuthorization To Release Medical CertificatePsychology TodayNo ratings yet
- PMRF RevisedDocument4 pagesPMRF RevisedacsalcedaNo ratings yet
- Member DeclarationDocument2 pagesMember Declarationchuzu123No ratings yet
- Carer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverDocument8 pagesCarer Payment and - or Carer Allowance Medical Report (SA332a) For A Person - 16 Years or OverWallace DunnNo ratings yet
- Mitgliedschaftsantrag Beschaeftigte - Englisch DataDocument1 pageMitgliedschaftsantrag Beschaeftigte - Englisch Datamicky johnNo ratings yet
- Federal Information Worksheet 2018: Jerry Pryde J JR 570-86-7356 DisabledDocument1 pageFederal Information Worksheet 2018: Jerry Pryde J JR 570-86-7356 Disabledsherrif douchebagNo ratings yet
- Health Insurance Quotation TemplateDocument1 pageHealth Insurance Quotation TemplatePrem KapoorNo ratings yet
- ESI Corporation e-Pehchan Card Provides Social Security BenefitsDocument3 pagesESI Corporation e-Pehchan Card Provides Social Security BenefitsSukhdeb BiswakarmaNo ratings yet
- OE Health Insurance Application 4 Fillable 1Document2 pagesOE Health Insurance Application 4 Fillable 1elena.e.rivelliNo ratings yet
- HMO Enrollment FormDocument2 pagesHMO Enrollment FormMarc ResuelloNo ratings yet
- Kawanihan NG Rentas Internas: Republika NG Pilipinas Kagawaran NG PananalapiDocument1 pageKawanihan NG Rentas Internas: Republika NG Pilipinas Kagawaran NG PananalapiPingLomaadEdulanNo ratings yet
- Ssa 3380 SampleDocument10 pagesSsa 3380 SampleAntiSocial CandiceNo ratings yet
- turito 2 (1)Document2 pagesturito 2 (1)M S SHARATHNo ratings yet
- Employee Waiver FormDocument1 pageEmployee Waiver FormL.A Review CenterNo ratings yet
- Mississippi State Board of Medical Licensure: Complaint FormDocument5 pagesMississippi State Board of Medical Licensure: Complaint FormScott SistersNo ratings yet
- Philhealth - Pag-Ibig MibDocument8 pagesPhilhealth - Pag-Ibig MibChino PaciaNo ratings yet
- Barrick Enrollment Form Apr 2022Document3 pagesBarrick Enrollment Form Apr 2022jorge ordinolaNo ratings yet
- Member Enrollment Application - APEX Plan - FillableDocument1 pageMember Enrollment Application - APEX Plan - Fillableeric.risnerNo ratings yet
- Labama Enior X: Client Intake FormDocument2 pagesLabama Enior X: Client Intake FormNicole FrederickNo ratings yet
- MHD app form (Trust)Document6 pagesMHD app form (Trust)mojija5822No ratings yet
- Bir Form 2305Document1 pageBir Form 2305MacneoNo ratings yet
- Proposal Form Yuva Bharat Health PolicyDocument7 pagesProposal Form Yuva Bharat Health PolicyVirendra VedNo ratings yet
- 18.medical Insurance Enrollment FormDocument2 pages18.medical Insurance Enrollment FormKratika PandeyNo ratings yet
- Newborn Application FormDocument2 pagesNewborn Application FormMicaela KrielNo ratings yet
- Consolidated Enrollment Form - SFI (FINAL-2018)Document2 pagesConsolidated Enrollment Form - SFI (FINAL-2018)Anh TranNo ratings yet
- Dependent Room and Board Benefit Limit Remarks/CategoryDocument6 pagesDependent Room and Board Benefit Limit Remarks/CategoryEdrick TarucNo ratings yet
- Family Financial QuestionnaireDocument4 pagesFamily Financial QuestionnaireAngela Miles Dizon0% (1)
- Client Information Sheet: Policy Owner Policy InsuredDocument2 pagesClient Information Sheet: Policy Owner Policy InsuredMae Mark TorresNo ratings yet
- GL 2002 140Document9 pagesGL 2002 140net2useNo ratings yet
- Anthem Medical Claim FormDocument2 pagesAnthem Medical Claim FormsaiprojectworkNo ratings yet
- Enrollment Short Form For Group InsuranceDocument1 pageEnrollment Short Form For Group InsuranceIra Angelo CorderoNo ratings yet
- Social Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceFrom EverandSocial Security: The New Rules, Essentials & Maximizing Your Social Security, Retirement, Medicare, Pensions & Benefits Explained In One PlaceNo ratings yet
- Guardianship Reality: Who’S Looking out for America’S Abandoned, Abused, Neglected Children & Elderly?From EverandGuardianship Reality: Who’S Looking out for America’S Abandoned, Abused, Neglected Children & Elderly?No ratings yet
- The Hidden Value in Your Life Insurance: Funds for Your RetirementFrom EverandThe Hidden Value in Your Life Insurance: Funds for Your RetirementNo ratings yet
- Family Child Care Legal and Insurance Guide: How to Protect Yourself from the Risks of Running a BusinessFrom EverandFamily Child Care Legal and Insurance Guide: How to Protect Yourself from the Risks of Running a BusinessNo ratings yet
- The Book of Answers for Federal Employees and Retirees - New 4th EditionFrom EverandThe Book of Answers for Federal Employees and Retirees - New 4th EditionNo ratings yet
- $Afer Income for Life: Couples May Qualify for up to $150,000 More in Social Security BenefitsFrom Everand$Afer Income for Life: Couples May Qualify for up to $150,000 More in Social Security BenefitsNo ratings yet
- How To Write A Successful CV1Document25 pagesHow To Write A Successful CV1steph T K S LNo ratings yet
- Business Letter Exercise Answer Sheet: HeadingDocument1 pageBusiness Letter Exercise Answer Sheet: Headingsteph T K S LNo ratings yet
- How To Write A Successful CV1Document25 pagesHow To Write A Successful CV1steph T K S LNo ratings yet
- Business PresentationsDocument19 pagesBusiness Presentationssteph T K S LNo ratings yet
- 3 Businessltr ExerciseDocument1 page3 Businessltr Exercisesteph T K S LNo ratings yet
- Business PresentationsDocument19 pagesBusiness Presentationssteph T K S LNo ratings yet
- Persuasive Letter Checklist: 8 TipsDocument1 pagePersuasive Letter Checklist: 8 Tipssteph T K S LNo ratings yet
- 2 PowerfulwordsDocument1 page2 Powerfulwordssteph T K S LNo ratings yet
- Teachingguide - Attention To Diversity and Educational Inclusion - Didactic ImplicationsDocument9 pagesTeachingguide - Attention To Diversity and Educational Inclusion - Didactic ImplicationsRichard Taylor PleiteNo ratings yet
- Property Law Course Manual Fall 2023Document16 pagesProperty Law Course Manual Fall 2023meghna22malikNo ratings yet
- An Overview of Paediatric SyndromesDocument50 pagesAn Overview of Paediatric SyndromesSana Bushra100% (11)
- Unit Iv - Children and Youth With Special Education NeedsDocument30 pagesUnit Iv - Children and Youth With Special Education NeedsMonalisa Benites Morales100% (1)
- Danielles Resume 2021Document5 pagesDanielles Resume 2021api-557506516No ratings yet
- Arvind General ReportDocument61 pagesArvind General ReportBirju PatelNo ratings yet
- Qahtani&Wyne TDJDocument5 pagesQahtani&Wyne TDJAmelia RosyidaNo ratings yet
- Sylabus - SPRT 102 - Sociology of North American SportDocument5 pagesSylabus - SPRT 102 - Sociology of North American Sportchris.douglas1No ratings yet
- PTSDDocument30 pagesPTSDVohn Andrae SarmientoNo ratings yet
- Issue 141Document4 pagesIssue 141Canowindra PhoenixNo ratings yet
- Study Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!Document2 pagesStudy Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!DoriNo ratings yet
- NIOS Admission Form - 2013-14Document4 pagesNIOS Admission Form - 2013-14distance_sanjeev100% (1)
- Qantas Disability Access Facilitation PlanDocument60 pagesQantas Disability Access Facilitation PlanFreddieNo ratings yet
- International Student Application Form: Privacy Statement Privacy NoticeDocument6 pagesInternational Student Application Form: Privacy Statement Privacy NoticeStella mariz DelarnaNo ratings yet
- 1 - 50 Ways Bias Fundamentals - English - v1 CompressedDocument67 pages1 - 50 Ways Bias Fundamentals - English - v1 CompressedMaryReyesNo ratings yet
- Equity Delighteth in EqualityDocument5 pagesEquity Delighteth in Equalitysyed jaffar aliNo ratings yet
- Aging in Place - From Theory To Practice PDFDocument12 pagesAging in Place - From Theory To Practice PDFYvonne Yap Ying Ying100% (1)
- Vergara v. Hammonia MaritimeDocument20 pagesVergara v. Hammonia MaritimeJohn BernalNo ratings yet
- Template For Clil Unit Plan For Teyl SensesDocument31 pagesTemplate For Clil Unit Plan For Teyl SensesSonia Felipe MartínezNo ratings yet
- Disability and Disability EvaluationDocument56 pagesDisability and Disability EvaluationAKHILNo ratings yet
- Bahir Dar University College of Education and Behavioral ScienceDocument36 pagesBahir Dar University College of Education and Behavioral ScienceFiteh KNo ratings yet
- Florence Blankenship v. Margaret M. Heckler, Secretary of Health and Human Services, 805 F.2d 393, 4th Cir. (1986)Document3 pagesFlorence Blankenship v. Margaret M. Heckler, Secretary of Health and Human Services, 805 F.2d 393, 4th Cir. (1986)Scribd Government DocsNo ratings yet
- Davison, Blankstein, Flett, Neale, Abnormal Psychology, 6th Canadian Edition TestbankDocument65 pagesDavison, Blankstein, Flett, Neale, Abnormal Psychology, 6th Canadian Edition TestbankMahin RahmanNo ratings yet
- Varayti NG Wika 12-47-1-PBDocument26 pagesVarayti NG Wika 12-47-1-PBAlmira Amor MarginNo ratings yet
- Mglva Student Handbook 2023-2024 FinalDocument66 pagesMglva Student Handbook 2023-2024 Finalapi-256528568No ratings yet
- Word of The DayDocument15 pagesWord of The DayReashiela LucenaNo ratings yet
- IND51207Document26 pagesIND51207Revathy MohanNo ratings yet