You might also like
- Air Compressor ManualDocument108 pagesAir Compressor ManualJhander BaluyotNo ratings yet
- Clinical Massage Therapy - S. Jurch Hill, 2009) WWDocument562 pagesClinical Massage Therapy - S. Jurch Hill, 2009) WWMohsen Bt92% (12)
- Knee Ligament InjuriesDocument5 pagesKnee Ligament InjuriesNijin XmxNo ratings yet
- Last Days of Diabetes Chaper 4Document39 pagesLast Days of Diabetes Chaper 4vtrackNo ratings yet
- Muscle Origin Insertion Innervation Action: (Branch of The Brachial Plexus)Document58 pagesMuscle Origin Insertion Innervation Action: (Branch of The Brachial Plexus)sdfs sdfdNo ratings yet
- HerniasDocument49 pagesHerniasAliNo ratings yet
- General Diet PlanDocument1 pageGeneral Diet PlanAzmat HusainNo ratings yet
- Pharmacovigilance DefinationsDocument32 pagesPharmacovigilance DefinationsKadir AmirNo ratings yet
- Daily Duas in The Month ofDocument258 pagesDaily Duas in The Month ofTransforNo ratings yet
- Resistant Hypertension. AHADocument38 pagesResistant Hypertension. AHAEderEmmanuelMartinezRuiz100% (1)
- Drawing Human FigureDocument128 pagesDrawing Human FigureMikeSufi100% (21)
- Lumbar Spine Trauma Imaging - Overview, Radiography, Computed TomographyDocument36 pagesLumbar Spine Trauma Imaging - Overview, Radiography, Computed TomographyAchmadRizaNo ratings yet
- The Most Common Causes of Eye Problems1Document4 pagesThe Most Common Causes of Eye Problems1shree ganeshNo ratings yet
- Hip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDocument38 pagesHip Joint: 5 December 2016 Anatomy Lecture By: DR Anita RaniDr'Dinesh MishraNo ratings yet
- Acl Injury Surgery - Orthoinfo - AaosDocument15 pagesAcl Injury Surgery - Orthoinfo - Aaosapi-228773845No ratings yet
- It's "ALL" in The Knees: A Review of The Anterolateral LigamentDocument16 pagesIt's "ALL" in The Knees: A Review of The Anterolateral LigamentAlMarcheseNo ratings yet
- CH 8: Skeletal System: Includes Bones, Cartilage and LigamentsDocument38 pagesCH 8: Skeletal System: Includes Bones, Cartilage and LigamentsMightyMouse1379No ratings yet
- Shoulder Dislocation Reduction TechniquesDocument71 pagesShoulder Dislocation Reduction TechniquesThành NPNo ratings yet
- ACL Injury: Does It Require Surgery?Document33 pagesACL Injury: Does It Require Surgery?Lee Woo GuanNo ratings yet
- AMD: What You Need to KnowDocument33 pagesAMD: What You Need to KnowtranzkulizerNo ratings yet
- Anterior Cruciate Ligament Tear DefinitionDocument8 pagesAnterior Cruciate Ligament Tear DefinitionEunice IquinaNo ratings yet
- All Dental AnatomyDocument114 pagesAll Dental AnatomyKhanh NguyễnNo ratings yet
- Complete Guide To ECGDocument78 pagesComplete Guide To ECGAnas YahyaNo ratings yet
- ACL InjuryDocument21 pagesACL InjuryVenkatesh Kandhaswamy RamalingamNo ratings yet
- Basic Examination of BloodDocument48 pagesBasic Examination of BloodmedinoNo ratings yet
- Swiss Ball Pike Ab WorkoutDocument9 pagesSwiss Ball Pike Ab WorkoutOana MozaNo ratings yet
- Cardiovascular Diagnostic Tests & Procedures.Document25 pagesCardiovascular Diagnostic Tests & Procedures.Salman KhanNo ratings yet
- SW Fantasy Companion GM InsertsDocument6 pagesSW Fantasy Companion GM InsertsMatt Cook100% (3)
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahNo ratings yet
- Knee Joint Inj and AspirationsDocument2 pagesKnee Joint Inj and AspirationsUmmu Nur FathonahNo ratings yet
- CXR Interpretation GuideDocument147 pagesCXR Interpretation GuideFcsieka FcseikaNo ratings yet
- Computer BasicDocument12 pagesComputer BasicanamikapariharNo ratings yet
- Al-Istighfaar (Seeking Forgiveness)Document8 pagesAl-Istighfaar (Seeking Forgiveness)MOHAMAD HANIM BIN MOHAMAD ISANo ratings yet
- WHO MDR 2020 Handbook Treatment PDFDocument88 pagesWHO MDR 2020 Handbook Treatment PDFYuanita GunawanNo ratings yet
- IV Fluid Types and UsesDocument6 pagesIV Fluid Types and UsesKiara Denise TamayoNo ratings yet
- Normal Radiographic Anatomical LandmarksDocument75 pagesNormal Radiographic Anatomical LandmarksDame rohanaNo ratings yet
- Acute Incisional Hernia: Theme From September 2011 ExamDocument146 pagesAcute Incisional Hernia: Theme From September 2011 ExamVimal Kumar YadavNo ratings yet
- Physical Assessment ResultDocument4 pagesPhysical Assessment Resultariskendell15No ratings yet
- Special Tests for Hip, Pelvis & Lower Extremity InjuriesDocument34 pagesSpecial Tests for Hip, Pelvis & Lower Extremity InjuriesFitri Isnaini100% (1)
- Common Diseases, Vol II - 1223Document214 pagesCommon Diseases, Vol II - 1223Farruh K100% (1)
- Elbow Fractures in PediatricsDocument57 pagesElbow Fractures in PediatricsKalaichelviRegunathan100% (1)
- Collateral Ligament Injuries - OrthoInfo - AAOSDocument4 pagesCollateral Ligament Injuries - OrthoInfo - AAOSgermanda yepezNo ratings yet
- Types of Common Knee Injuries ExplainedDocument6 pagesTypes of Common Knee Injuries ExplainedSagarNo ratings yet
- 14) PPT ROMAN Salah Training - StudentsDocument342 pages14) PPT ROMAN Salah Training - Studentsamer sohailNo ratings yet
- The 5 Most Common Sports InjuriesDocument4 pagesThe 5 Most Common Sports InjuriesAngeline SahagunNo ratings yet
- Key Board Short CutDocument6 pagesKey Board Short CutChaitanya KumarNo ratings yet
- Eye Path12Document45 pagesEye Path12JillKellyNo ratings yet
- Vitamin Deficiency and Food Recommendation System Using Machine LearningDocument10 pagesVitamin Deficiency and Food Recommendation System Using Machine LearningIJRASETPublicationsNo ratings yet
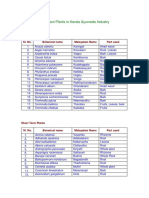
- Important Plants in Kerala Ayurveda Industry: Tree CropsDocument2 pagesImportant Plants in Kerala Ayurveda Industry: Tree Cropsajeez86No ratings yet
- Rectal ProlapseDocument6 pagesRectal ProlapseAnjani Putri RetnaninggalihNo ratings yet
- Ragay - Notes of EentDocument15 pagesRagay - Notes of Eentaynin39No ratings yet
- Vision Technician FGDocument361 pagesVision Technician FGDr Anchal GuptaNo ratings yet
- What Is Being Tested?: White Blood CellsDocument48 pagesWhat Is Being Tested?: White Blood Cellsstudent_019No ratings yet
- Carbohydrate Metabolism Disorders Stom 10-11Document61 pagesCarbohydrate Metabolism Disorders Stom 10-11Artem GrigoryanNo ratings yet
- Development of Hemorrhoids: Anal Canal AnatomyDocument20 pagesDevelopment of Hemorrhoids: Anal Canal AnatomyKris TejereroNo ratings yet
- Test Report Gupta DiagnosisDocument17 pagesTest Report Gupta Diagnosisdrblgupta1973100% (1)
- Common Dental ProblemsDocument14 pagesCommon Dental ProblemsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Frozen Shoulder: Presented By:Anubhav Verma Chairperson: Dr. Pramod BM 9 June 2015Document71 pagesFrozen Shoulder: Presented By:Anubhav Verma Chairperson: Dr. Pramod BM 9 June 2015Frensi Ayu PrimantariNo ratings yet
- What's New in Respiratory DisordersDocument4 pagesWhat's New in Respiratory DisorderssobanNo ratings yet
- TELEKOMUNIKASI DAN KOMPUTER RANGKAIANDocument19 pagesTELEKOMUNIKASI DAN KOMPUTER RANGKAIANAmer IkhwanNo ratings yet
- Widal Agglutination Test PDFDocument5 pagesWidal Agglutination Test PDFशशांक तिवारीNo ratings yet
- Ent Hearing Tests, Vestibular TestsDocument13 pagesEnt Hearing Tests, Vestibular TestsSuleman MuhammadNo ratings yet
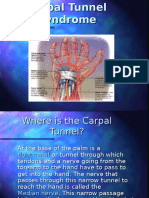
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeselviagandasariNo ratings yet
- Fracture Colles Rehabilitation Advice Following WristDocument4 pagesFracture Colles Rehabilitation Advice Following WristfaprilisaNo ratings yet
- Plantar Fasciitis - A Self Help GuideDocument8 pagesPlantar Fasciitis - A Self Help GuideAjmera HarshalNo ratings yet
- Anatomy FootDocument22 pagesAnatomy Footazis aimaduddinNo ratings yet
- Cardiotonic DrugsDocument67 pagesCardiotonic DrugsLady Mae Ramos100% (1)
- Claw HandDocument54 pagesClaw HandNibu Kurian67% (3)
- Physics Problems Chp6Document2 pagesPhysics Problems Chp6snottlebieNo ratings yet
- Physics ProblemsDocument4 pagesPhysics ProblemssnottlebieNo ratings yet
- Physics Problems Chp14Document2 pagesPhysics Problems Chp14snottlebieNo ratings yet
- Physics ProblemsDocument4 pagesPhysics ProblemssnottlebieNo ratings yet
- Hague Street Explosion 1850Document3 pagesHague Street Explosion 1850Jaya Mae MañagoNo ratings yet
- Just-in-Time Lecture: China Earthquake: 12 May 2008Document58 pagesJust-in-Time Lecture: China Earthquake: 12 May 2008Ana-Maria LucaNo ratings yet
- LP Radius Ulna FractureDocument22 pagesLP Radius Ulna FractureMuhammad PanduNo ratings yet
- Background ResearchDocument5 pagesBackground ResearchNordiana IdrisNo ratings yet
- Blunt Force Trauma: Slide 1Document19 pagesBlunt Force Trauma: Slide 1Achmad MuflihNo ratings yet
- En Do Don Tic Orthodontic Relationship Are View of Treatment Planning ChangesDocument18 pagesEn Do Don Tic Orthodontic Relationship Are View of Treatment Planning ChangesSatpal SandhuNo ratings yet
- MR Supple All 2014Document429 pagesMR Supple All 2014Regita Ayu LestariNo ratings yet
- HEALTH RECORD REVIEWDocument2 pagesHEALTH RECORD REVIEWJA BerzabalNo ratings yet
- Human Reflex Physiology: ExerciseDocument4 pagesHuman Reflex Physiology: ExerciseGlainee esor selfroNo ratings yet
- Ankylosing Modalities (Aks) : Costovertebral Joints Are Effected, Kyphosis Can Occur and Alter RespDocument16 pagesAnkylosing Modalities (Aks) : Costovertebral Joints Are Effected, Kyphosis Can Occur and Alter RespCynthia L Hovland- GeracieNo ratings yet
- 113034153s 45971675 254009105 Causeeffect Essay Final DraftDocument6 pages113034153s 45971675 254009105 Causeeffect Essay Final Draftapi-320097699No ratings yet
- Another League - CaraNoDocument86 pagesAnother League - CaraNocasajana100% (2)
- Careplan Week 8Document3 pagesCareplan Week 8api-353681121No ratings yet
- Clinical Anatomy of The Anterior Abdominal Wall in Its Relation To HerniaDocument23 pagesClinical Anatomy of The Anterior Abdominal Wall in Its Relation To HerniaLytiana WilliamsNo ratings yet
- NUTRICOOK Smart Pot Manual BookDocument52 pagesNUTRICOOK Smart Pot Manual BookszsoomroNo ratings yet
- OSTEOLOGY OF THE THORAXDocument68 pagesOSTEOLOGY OF THE THORAXINTERNET MONEY HACKNo ratings yet
- Napfa Resource Book For Pe Teachers 20140506Document25 pagesNapfa Resource Book For Pe Teachers 20140506api-259265137100% (1)
- Basic First Aid Manual EnglishDocument44 pagesBasic First Aid Manual Englisharold bodoNo ratings yet
- HLTH9 - 3Q First Aid For Common Unintentional InjuriesDocument5 pagesHLTH9 - 3Q First Aid For Common Unintentional InjuriesNardriel Kinsley TrongcosoNo ratings yet
- Thunder Ball ScriptDocument20 pagesThunder Ball ScriptKeng ThioNo ratings yet
- Telaah Jurnal KGDDocument17 pagesTelaah Jurnal KGDriska eka fatma HasibuanNo ratings yet
- Foot DropDocument2 pagesFoot DropSaravanan SridharanNo ratings yet