You might also like
- Stage 4 Gastric Cancer Case PresentationDocument61 pagesStage 4 Gastric Cancer Case PresentationsandeepNo ratings yet
- Update On Gastric AJCC 8th EdDocument42 pagesUpdate On Gastric AJCC 8th EdBenNo ratings yet
- Treatment Options for Gastric AdenocarcinomaDocument45 pagesTreatment Options for Gastric AdenocarcinomaajNo ratings yet
- Esophageal Carcinoma: Mark Louie M. Lanting, MDDocument44 pagesEsophageal Carcinoma: Mark Louie M. Lanting, MDlouie10279098No ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Rectal Carcinoma and Colonic Polyps ReviewDocument62 pagesRectal Carcinoma and Colonic Polyps ReviewSK TalkNo ratings yet
- Gastriccancer 160428190410Document54 pagesGastriccancer 160428190410Pranavi ShewaleNo ratings yet
- Urinary Bladder Neoplasm: DR Rikesh Jung Karkee Assitant Professor Urology Division Surgery DepartmentDocument60 pagesUrinary Bladder Neoplasm: DR Rikesh Jung Karkee Assitant Professor Urology Division Surgery DepartmentAashish YadavNo ratings yet
- CarcinomarectumDocument45 pagesCarcinomarectumHuzefa MemonNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- Testicular Tumors The EndDocument67 pagesTesticular Tumors The EndRamesh ReddyNo ratings yet
- Pancreatic Nursing Oncologic NursingDocument15 pagesPancreatic Nursing Oncologic NursingMari ManlapazNo ratings yet
- Surgery Bladder TumorDocument35 pagesSurgery Bladder TumorMuhammad ArsalNo ratings yet
- Thyroid Cancer and It's Management: Dr. Nurun Nahar CMO Head, Thyroid Division InmuDocument44 pagesThyroid Cancer and It's Management: Dr. Nurun Nahar CMO Head, Thyroid Division InmuParvez AhmedNo ratings yet
- Kidney Cancer: Earnest John B. Tenorio, MD, DPBSDocument32 pagesKidney Cancer: Earnest John B. Tenorio, MD, DPBSAbishek PrinceNo ratings yet
- Gastric CancerDocument65 pagesGastric CanceranandtmcNo ratings yet
- Management of Rectal Cancer... by DR Kassahun GirmaDocument50 pagesManagement of Rectal Cancer... by DR Kassahun GirmaKassahun Girma Gelaw100% (1)
- G.I Tumors-1 Esophagus and StomachDocument53 pagesG.I Tumors-1 Esophagus and StomachAjeet LohanaNo ratings yet
- Gastric Carcinoma: Dr. Gautam DasDocument45 pagesGastric Carcinoma: Dr. Gautam DasRajarshi KumarNo ratings yet
- Esophageal CarcinomaDocument34 pagesEsophageal Carcinomaapi-19916399100% (1)
- Management of Thyroid CancerDocument57 pagesManagement of Thyroid CancerAshis SahaNo ratings yet
- MalarDocument41 pagesMalarமணிகண்டன் ராஜேந்திரன்No ratings yet
- CasediscussionDocument30 pagesCasediscussionFernando AnibanNo ratings yet
- Role of Radiotherapy For Hepatocellular CarcinomaDocument37 pagesRole of Radiotherapy For Hepatocellular CarcinomabahtiarhabibiNo ratings yet
- Ovarian Cancer SGTDocument25 pagesOvarian Cancer SGTAndre PutraNo ratings yet
- Colorectal CancerDocument39 pagesColorectal CancerFernando AnibanNo ratings yet
- Gall Bladder CarcinomaDocument29 pagesGall Bladder CarcinomaUsman FarooqNo ratings yet
- Gis 1 EnglishDocument85 pagesGis 1 Englishexand861No ratings yet
- Management of Wilms Tumor: Literature Review (NAMA)Document15 pagesManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- 20.MBBS Pancreatic CancerDocument52 pages20.MBBS Pancreatic Cancermrajah95No ratings yet
- Peritoneal Carcinomatosis Recent Advances in Surgery - 16 Edition Roshanlal GuptaDocument48 pagesPeritoneal Carcinomatosis Recent Advances in Surgery - 16 Edition Roshanlal GuptaPraveen CpNo ratings yet
- Lower Gi Case Presentation PDFDocument35 pagesLower Gi Case Presentation PDFapi-448999672No ratings yet
- CA Gall BladderDocument24 pagesCA Gall BladderTheoder RobinsonNo ratings yet
- Gastriccancer 170426015531Document124 pagesGastriccancer 170426015531meftuh abdiNo ratings yet
- Rectal CancerDocument39 pagesRectal CancerKeam PisethsapheareachNo ratings yet
- Rectal Cancer Talk 1228785749826555 9Document54 pagesRectal Cancer Talk 1228785749826555 9Jantima SirisophonwattanaNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- Pancreatic Cancer: Dr. Tjatur Winarsanto SPPDDocument41 pagesPancreatic Cancer: Dr. Tjatur Winarsanto SPPDMayiz Renata LimerseNo ratings yet
- Management of Endometrial CarcinomaDocument46 pagesManagement of Endometrial CarcinomaSapna SNo ratings yet
- Management of Lung Cancer by DR Abdul-AzizDocument89 pagesManagement of Lung Cancer by DR Abdul-AzizAbdulaziz HassenNo ratings yet
- Basics of GI Cancer Radiation Therapy Planning, Delivery and Motion ManagementDocument77 pagesBasics of GI Cancer Radiation Therapy Planning, Delivery and Motion ManagementgammasharkNo ratings yet
- Gastric Cancer Staging, Risk Factors, and Treatment OptionsDocument36 pagesGastric Cancer Staging, Risk Factors, and Treatment Optionsnancy voraNo ratings yet
- L1 GIT OncologyDocument99 pagesL1 GIT OncologyPrincess FNo ratings yet
- Pancreas LiverDocument21 pagesPancreas LiverSarfaraz ansariNo ratings yet
- Common Bile Duct Stones StrictureDocument48 pagesCommon Bile Duct Stones StrictureSyarif MalawatNo ratings yet
- Ghid American 2015 ScurtDocument33 pagesGhid American 2015 ScurtMissButterfly03No ratings yet
- Carcinoma StomachDocument24 pagesCarcinoma StomachHemanth MakineniNo ratings yet
- Benign Tumors Adenomas (Most Common Benign Neoplasm) :: True Adenomas: Ileum Villous Adenoma: DuodenumDocument8 pagesBenign Tumors Adenomas (Most Common Benign Neoplasm) :: True Adenomas: Ileum Villous Adenoma: DuodenumTheeya QuigaoNo ratings yet
- Atypical Colorectal NeoplasmsDocument52 pagesAtypical Colorectal NeoplasmsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- UTUCDocument39 pagesUTUCShalini shreeNo ratings yet
- Anal Canal CarcinomaDocument24 pagesAnal Canal CarcinomaArun guruNo ratings yet
- Ca Colon: Pembimbing Dr. Yanti, SP.B KBDDocument47 pagesCa Colon: Pembimbing Dr. Yanti, SP.B KBDRichard HadinataNo ratings yet
- Principles of Surgical OncologyDocument34 pagesPrinciples of Surgical Oncologykaukab azim100% (1)
- 3-3-08 KnudsonDocument27 pages3-3-08 KnudsonNurRahmaMusdalifaNo ratings yet
- Oesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHDocument50 pagesOesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHMalgh Kh100% (2)
- Management of Colon Cancers-1Document110 pagesManagement of Colon Cancers-1Edwin OkonNo ratings yet
- Colorectal TumoursDocument21 pagesColorectal TumoursRUDOLF YUSON BM20110052No ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- EulaDocument3 pagesEulaBrandon YorkNo ratings yet
- Fortiap v6.0.5 Upgrade Table PDFDocument2 pagesFortiap v6.0.5 Upgrade Table PDFtorr123No ratings yet
- DGFT IndiaDocument33 pagesDGFT IndiaKarthik RedNo ratings yet
- Fortiap S Fortiap w2 v6.0.5 Release Notes PDFDocument10 pagesFortiap S Fortiap w2 v6.0.5 Release Notes PDFtorr123No ratings yet
- Dr. Praveen Kumar DoddamaniDocument81 pagesDr. Praveen Kumar Doddamanitorr123100% (2)
- Bonetumoursandprinciplesoflimbsalvagesurgery 140504075940 Phpapp01Document87 pagesBonetumoursandprinciplesoflimbsalvagesurgery 140504075940 Phpapp01torr123No ratings yet
- Understanding Parkinson's DiseaseDocument52 pagesUnderstanding Parkinson's Diseasetorr123No ratings yet
- EEM Best PracticesDocument26 pagesEEM Best Practicestorr123No ratings yet
- DGFT IndiaDocument33 pagesDGFT IndiaKarthik RedNo ratings yet
- Presented By: Dr. Vishal Bathma Asst. Professor Community Medicine PCMS&RCDocument42 pagesPresented By: Dr. Vishal Bathma Asst. Professor Community Medicine PCMS&RCtorr123No ratings yet
- Hypertension: PharmacotherapyDocument23 pagesHypertension: Pharmacotherapytorr123No ratings yet
- Vishnu Priya Anguraj Tsmu Grp-14Document39 pagesVishnu Priya Anguraj Tsmu Grp-14torr123100% (1)
- Contactdermatitis 130920140849 Phpapp01Document65 pagesContactdermatitis 130920140849 Phpapp01torr123No ratings yet
- Cranial Osteomyelitis Diagnosis and Treatment OptionsDocument5 pagesCranial Osteomyelitis Diagnosis and Treatment OptionsRajanish Kumar50% (2)
- Management of Unconscious PatientDocument51 pagesManagement of Unconscious PatientEmenike Donald Ejieji50% (2)
- Administration Guide: 17 February 2013Document303 pagesAdministration Guide: 17 February 2013torr123No ratings yet
- Preventing AFib Related Strokes SlideDocument48 pagesPreventing AFib Related Strokes Slidetorr123No ratings yet
- UnconsciousnessDocument91 pagesUnconsciousnessFitri Amelia RizkiNo ratings yet
- HaemodialysisDocument98 pagesHaemodialysisKo Zin100% (1)
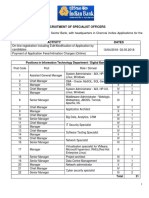
- India Bank Recruitment of Specialist Officers EngDocument25 pagesIndia Bank Recruitment of Specialist Officers Engajay kumarNo ratings yet
- CP R75.40VS SmartViewTracker AdminGuideDocument31 pagesCP R75.40VS SmartViewTracker AdminGuidetorr123No ratings yet
- Afib574903profslideshareversiondaspeakerbureauslidedeck10 131017131248 Phpapp02Document31 pagesAfib574903profslideshareversiondaspeakerbureauslidedeck10 131017131248 Phpapp02torr123No ratings yet
- Preventing AFib Related Strokes SlideDocument48 pagesPreventing AFib Related Strokes Slidetorr123No ratings yet
- India Bank Recruitment of Specialist Officers EngDocument25 pagesIndia Bank Recruitment of Specialist Officers Engajay kumarNo ratings yet
- Hspowerpoint 140424161028 Phpapp01Document25 pagesHspowerpoint 140424161028 Phpapp01torr123No ratings yet
- CP R75.40VS SmartViewTracker AdminGuideDocument31 pagesCP R75.40VS SmartViewTracker AdminGuidetorr123No ratings yet
- Liver Diseases With Pregnancy3603Document138 pagesLiver Diseases With Pregnancy3603torr123No ratings yet
- Physiological Aspect of Foods & Drugs As Aphrodisiacs: Guided By-Presented byDocument21 pagesPhysiological Aspect of Foods & Drugs As Aphrodisiacs: Guided By-Presented bytorr123No ratings yet
- CCNP Work BookDocument94 pagesCCNP Work Booktorr123100% (1)
- Meningitis Beyond Neonatal AgeDocument57 pagesMeningitis Beyond Neonatal AgeTilahun Kegne100% (2)
- Gerunds: A verb form ending in -ing that can act as a noun, adjective or verbDocument29 pagesGerunds: A verb form ending in -ing that can act as a noun, adjective or verbOLIVER JACS SAENZ SERPANo ratings yet
- ICU-Acquired Weakness and Recovery From Critical IllnessDocument9 pagesICU-Acquired Weakness and Recovery From Critical IllnessFebrian ParuraNo ratings yet
- Psych 10Document10 pagesPsych 10karenkaren09No ratings yet
- IV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneDocument2 pagesIV Induction Agents: Propofol, Ketamine, Etomidate, ThiopentoneNdalilashiwa Penehafo Ndakondja-VictorNo ratings yet
- Daptomycin (Cubicin)Document1 pageDaptomycin (Cubicin)Adrianne BazoNo ratings yet
- Trauma Brain Injury, Kuliah PakarDocument40 pagesTrauma Brain Injury, Kuliah PakarveninoriaNo ratings yet
- DJFMH - PPT.01.05.2016 (2003)Document55 pagesDJFMH - PPT.01.05.2016 (2003)Angellaine Bulanadi100% (1)
- Mucogingival SurgeryDocument53 pagesMucogingival SurgeryAbhijeet Shete100% (3)
- SerologyDocument33 pagesSerologyGEBEYAW ADDISUNo ratings yet
- Vaginal Yeast InfectionsDocument7 pagesVaginal Yeast InfectionsAnimesh PriyaNo ratings yet
- Er LFD 11Document1 pageEr LFD 11EldwinCauilanNo ratings yet
- Case Report Consent Form TemplateDocument2 pagesCase Report Consent Form TemplateDaniel Antonio Valderrama Merejildo100% (1)
- Salient Features - MPPRC DIARRHEA RevisedDocument12 pagesSalient Features - MPPRC DIARRHEA RevisedLui Yalong Jr.No ratings yet
- Agen HematinikDocument77 pagesAgen HematinikErinaGeraldiNo ratings yet
- Nagrik Suraksha Individual Policy SummaryDocument10 pagesNagrik Suraksha Individual Policy SummarypayalNo ratings yet
- Nursing Assessment For PainDocument9 pagesNursing Assessment For PainNDJNo ratings yet
- TriageDocument42 pagesTriageNic JiNo ratings yet
- ObjectivesDocument2 pagesObjectivesAmy RamirezNo ratings yet
- Peads - Diamond Blackfan AnemiaDocument40 pagesPeads - Diamond Blackfan AnemiaBaran PalanimuthuNo ratings yet
- MediShield Life: Better Protection for AllDocument20 pagesMediShield Life: Better Protection for Alljakovach7No ratings yet
- Annex G - Infection Control Annual Plan 2012-13Document7 pagesAnnex G - Infection Control Annual Plan 2012-13Tianti PuadiNo ratings yet
- Short Sightedness Vs Long SightDocument1 pageShort Sightedness Vs Long SightDevill DavajNo ratings yet
- Bio Equivalence Study of Tizanidine HCL Tablets 4 MG of DR - Reddys Under Fasting Conditions - Full Text View - Clinical TrialsDocument4 pagesBio Equivalence Study of Tizanidine HCL Tablets 4 MG of DR - Reddys Under Fasting Conditions - Full Text View - Clinical TrialsMuhammad Hafeez ArainNo ratings yet
- Gallstones: American College of Gastroenterology Common Gastrointestinal ProblemsDocument2 pagesGallstones: American College of Gastroenterology Common Gastrointestinal ProblemsanonNo ratings yet
- Saint Alphonsus Statement On LettersDocument1 pageSaint Alphonsus Statement On LettersKBOI 2NewsNo ratings yet
- Gastrointestinal and Esophageal Foreign Bodies in The Dog and CatDocument5 pagesGastrointestinal and Esophageal Foreign Bodies in The Dog and CatMuh Iqbal DjamilNo ratings yet
- Perioperative Nursing Care IssuesDocument7 pagesPerioperative Nursing Care IssuesAziil LiizaNo ratings yet
- Full Mouth RehabDocument37 pagesFull Mouth RehabAravind Krishnan100% (4)
- How to Disengage from "Sensorimotor ObsessionsDocument5 pagesHow to Disengage from "Sensorimotor Obsessionsbferrreira2371100% (1)