You might also like
- The Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsFrom EverandThe Ultimate Guide to Vascular Ultrasound: Diagnosing and Understanding Vascular ConditionsNo ratings yet
- Surgical Outcomes of Varicose Veins at Universal College of Medical SciencesDocument3 pagesSurgical Outcomes of Varicose Veins at Universal College of Medical SciencesLusiNo ratings yet
- Venous DiseaseDocument50 pagesVenous Diseaseعرفان رفعت پناهNo ratings yet
- Management of Chronic Venous Disease: 7th Annual Women's Heart & Vascular SymposiumDocument3 pagesManagement of Chronic Venous Disease: 7th Annual Women's Heart & Vascular Symposiumatika5No ratings yet
- Definition, Presentation, Treatment, and Histology: by Dr. Martin Mihm, Jr. and Linda Rozell-Shannon, M.SDocument17 pagesDefinition, Presentation, Treatment, and Histology: by Dr. Martin Mihm, Jr. and Linda Rozell-Shannon, M.SAriandindi AriandiNo ratings yet
- Hemodynamics and Diagnosis Venous Disease-Jvs 1207Document21 pagesHemodynamics and Diagnosis Venous Disease-Jvs 1207Fahrudin ŠabanovićNo ratings yet
- Imaging Classification of Vascular MalformationsDocument16 pagesImaging Classification of Vascular MalformationsHector Hernandez-SoriaNo ratings yet
- Visceral Aneurysms - Old Paradigms, New Insights? PDFDocument8 pagesVisceral Aneurysms - Old Paradigms, New Insights? PDFYasir BouchiNo ratings yet
- Arteriovenous Malformations of The Body and Extremities: Analysis of Therapeutic Outcomes andDocument12 pagesArteriovenous Malformations of The Body and Extremities: Analysis of Therapeutic Outcomes andClaudio SalazarNo ratings yet
- Analisis Guias Valvulas ESCDocument9 pagesAnalisis Guias Valvulas ESCCamiloRadaNo ratings yet
- PIIS091450871930084XDocument7 pagesPIIS091450871930084XdrewantaNo ratings yet
- Rutman Et Al 2022 Incidental Vascular Findings On Brain Magnetic Resonance AngiographyDocument13 pagesRutman Et Al 2022 Incidental Vascular Findings On Brain Magnetic Resonance AngiographySofía ValdésNo ratings yet
- 6th Year AVM, Anurysm, Venous and LymphaticDocument103 pages6th Year AVM, Anurysm, Venous and LymphaticamrNo ratings yet
- Cu 19 7Document6 pagesCu 19 701-13-07 G.No ratings yet
- ThrombophlebitisDocument3 pagesThrombophlebitismirrejNo ratings yet
- Brain Arteriovenous MalformationsDocument20 pagesBrain Arteriovenous MalformationsTony NgNo ratings yet
- Doppler Venoso MMIIDocument23 pagesDoppler Venoso MMIIAdriana KimuraNo ratings yet
- CSM_3_2_46_52Document7 pagesCSM_3_2_46_52Santoso 9JimmyNo ratings yet
- Surgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromeDocument8 pagesSurgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromenikitagustiNo ratings yet
- Tugas PDDocument59 pagesTugas PDfirmanNo ratings yet
- Vascular Malformations of The Central Nervous SystemDocument9 pagesVascular Malformations of The Central Nervous SystemFranklin Aranda100% (2)
- Di Napoli Et Al 2020 Arterial Spin Labeling Mri in Carotid Stenosis Arterial Transit Artifacts May Predict SymptomsDocument9 pagesDi Napoli Et Al 2020 Arterial Spin Labeling Mri in Carotid Stenosis Arterial Transit Artifacts May Predict SymptomsAdenane BoussoufNo ratings yet
- Management of True Aneurysms of Hemodialysis Access FistulasDocument7 pagesManagement of True Aneurysms of Hemodialysis Access FistulasbobbyNo ratings yet
- Low Flow Vascular Malformations ManagementDocument23 pagesLow Flow Vascular Malformations ManagementVedarth DashNo ratings yet
- CardiologyDocument11 pagesCardiologyandreaNo ratings yet
- Guia Uciq PlaquetopeniaDocument6 pagesGuia Uciq PlaquetopeniaAmanqui Alex DerlyNo ratings yet
- Ecr2015 C-0778Document19 pagesEcr2015 C-0778Violet HillNo ratings yet
- Imaging and Management of Vascular MalformationsDocument11 pagesImaging and Management of Vascular MalformationsMessah V DianaNo ratings yet
- Hybrid Coronary Revascularization: Promising, But Yet To Take OffDocument13 pagesHybrid Coronary Revascularization: Promising, But Yet To Take OffSherZalattha KuchikiElfNo ratings yet
- Uw Step3 NotesDocument34 pagesUw Step3 NotesAakash ShahNo ratings yet
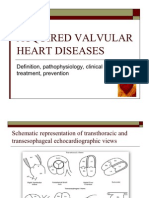
- Acquired Valvular Heart DiseaseDocument73 pagesAcquired Valvular Heart DiseaseYash TripathiNo ratings yet
- Uncorrected Author ProofDocument18 pagesUncorrected Author ProofClaudio SalazarNo ratings yet
- Orbital AVMDocument7 pagesOrbital AVMDedeh KurniasihNo ratings yet
- Diseases of The AortaDocument48 pagesDiseases of The AortaYibeltal AssefaNo ratings yet
- Consenso Europeo Del Manejo y DX de La Displasia Fibromuscular 2014Document12 pagesConsenso Europeo Del Manejo y DX de La Displasia Fibromuscular 2014Diego Andrés Mejía VascoNo ratings yet
- Loukas 2013Document11 pagesLoukas 2013Gabriel Jose CarvajalNo ratings yet
- Cvi ZamboniDocument14 pagesCvi ZambonienzofracchiaNo ratings yet
- Analysis of 1,338 Patients with Acute Lower Limb DVTDocument6 pagesAnalysis of 1,338 Patients with Acute Lower Limb DVTBeby Dwi Lestari BajryNo ratings yet
- E-Poster Mumbai FinalDocument5 pagesE-Poster Mumbai FinalSuman SagarNo ratings yet
- 1-s2.0-S0741521416318535-mainDocument11 pages1-s2.0-S0741521416318535-mainRohib MalikNo ratings yet
- Vascular Tumors: Infantile HemangiomaDocument4 pagesVascular Tumors: Infantile HemangiomavicenteturasNo ratings yet
- Minimally Invasive Treatments For Perforator Vein InsufficiencyDocument6 pagesMinimally Invasive Treatments For Perforator Vein Insufficiencyatika5No ratings yet
- Unusual May-Thurner Syndrome CaseDocument5 pagesUnusual May-Thurner Syndrome CaseJ. Ruben HermannNo ratings yet
- Jurnal Coronary Artery FistulaDocument3 pagesJurnal Coronary Artery FistulaRistinyaUnuyNo ratings yet
- Hypoxia and Complications of Oxygenation in Extracorporeal Membrane OxygenationDocument7 pagesHypoxia and Complications of Oxygenation in Extracorporeal Membrane Oxygenationjq4rhbh2pzNo ratings yet
- Pathophysiology and Diagnosis of Deep Venous ThrombosisDocument12 pagesPathophysiology and Diagnosis of Deep Venous ThrombosisLuisa RuizNo ratings yet
- Dad 0000000000000141Document7 pagesDad 0000000000000141Kaleab YinebebalNo ratings yet
- Review Trombosis CerebrovascularDocument10 pagesReview Trombosis CerebrovascularDiego Velásquez HerreraNo ratings yet
- Jurnal InternalDocument10 pagesJurnal InternalseptikusumaNo ratings yet
- MR-6 - Valvular Surgery-2021. StudDocument34 pagesMR-6 - Valvular Surgery-2021. StudShruti JestineNo ratings yet
- MAHA Diagnosis and Management in TTP and HUS - A ReviewDocument14 pagesMAHA Diagnosis and Management in TTP and HUS - A ReviewRachmi FadillahNo ratings yet
- Superior Vena Cava Syndrome WewwDocument8 pagesSuperior Vena Cava Syndrome WewwIgnatius Yuwanda ChrissanderNo ratings yet
- Jurnal DinaDocument11 pagesJurnal DinaRahma Puji LestariNo ratings yet
- Imagen Hepática Vascular Hígado 2022Document15 pagesImagen Hepática Vascular Hígado 2022Oscar BushNo ratings yet
- Porto-Systemic Shunts: Classification, Clinical and Radiological ImplicationsDocument39 pagesPorto-Systemic Shunts: Classification, Clinical and Radiological ImplicationsSyifa SalsabilaNo ratings yet
- Arteriovenous MalformationsDocument24 pagesArteriovenous MalformationsfachrurroziNo ratings yet
- Venous Thromboembolism DiseaseDocument49 pagesVenous Thromboembolism DiseaseNiko YuandikaNo ratings yet
- Venous ThromboembolismDocument28 pagesVenous ThromboembolismValeria MolinaNo ratings yet
- Jurnal NurulDocument22 pagesJurnal NurulGaling Chandika PutraNo ratings yet
- Intra Aortic Balloon Pump (IABP) 2009Document57 pagesIntra Aortic Balloon Pump (IABP) 2009nurminsyahNo ratings yet
- Chen 2015Document6 pagesChen 2015nurminsyahNo ratings yet
- Hiponatremia in CHFDocument5 pagesHiponatremia in CHFnurminsyahNo ratings yet
- Anatomy PDFDocument163 pagesAnatomy PDFnurminsyahNo ratings yet
- EF4Document3 pagesEF4FugerMahdeneM'psrNo ratings yet
- Imaging AVMDocument5 pagesImaging AVMnurminsyahNo ratings yet
- Ferreiro Et Al 2016Document18 pagesFerreiro Et Al 2016nurminsyahNo ratings yet
- EF4Document3 pagesEF4FugerMahdeneM'psrNo ratings yet
- Peripheral Vascular ExaminationDocument27 pagesPeripheral Vascular ExaminationnurminsyahNo ratings yet
- Treatment of High-Flow Arteriovenous MalformationsDocument9 pagesTreatment of High-Flow Arteriovenous MalformationsnurminsyahNo ratings yet
- Avm TheraphyDocument12 pagesAvm TheraphynurminsyahNo ratings yet
- Radiologi Aneurisma AortaDocument11 pagesRadiologi Aneurisma AortanurminsyahNo ratings yet
- Imaging AVMDocument5 pagesImaging AVMnurminsyahNo ratings yet
- LE Diagnosis and ManagementDocument14 pagesLE Diagnosis and ManagementnurminsyahNo ratings yet
- Diagnosisfor PEDocument28 pagesDiagnosisfor PEMohd Syaiful Mohd ArisNo ratings yet
- Avm TheraphyDocument12 pagesAvm TheraphynurminsyahNo ratings yet
- Cardiology Ultrasound EmergencyDocument92 pagesCardiology Ultrasound Emergencybeeluvit81444No ratings yet
- Cardiology Ultrasound EmergencyDocument92 pagesCardiology Ultrasound Emergencybeeluvit81444No ratings yet
- Brochure Mostacareup GBDocument9 pagesBrochure Mostacareup GBAroelNo ratings yet
- Internal Medicine PDFDocument76 pagesInternal Medicine PDFroxxanaNo ratings yet
- Physiology Lecture 10 Q-Bank (Cardiac Muscle - Action Potentials)Document15 pagesPhysiology Lecture 10 Q-Bank (Cardiac Muscle - Action Potentials)ChrisOrtNo ratings yet
- Mechanisms of Cardiac Arrhythmias From Automatici+Document24 pagesMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanNo ratings yet
- Calcibloc ODDocument2 pagesCalcibloc ODianecunarNo ratings yet
- Jurnal Cardiac RhabdomyomaDocument12 pagesJurnal Cardiac Rhabdomyomamagda goeyNo ratings yet
- BVCCT-304 EchocardiographyDocument71 pagesBVCCT-304 EchocardiographyManisha khanNo ratings yet
- DCM - Heart Failure Due to Dilated CardiomyopathyDocument13 pagesDCM - Heart Failure Due to Dilated CardiomyopathyPrincysuzine PintoNo ratings yet
- Cardiac Anatomy Physiology Blood Flow HeartDocument1 pageCardiac Anatomy Physiology Blood Flow HeartTori RolandNo ratings yet
- Circulatory System IGCSE Biology Notes and Questions 1Document4 pagesCirculatory System IGCSE Biology Notes and Questions 1Muhammad IbraheemNo ratings yet
- 3 - Series 2022Document9 pages3 - Series 2022Vijay UNo ratings yet
- Inotul Si InimaDocument8 pagesInotul Si InimaMihail RonnyNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Cardiac Cycle: Mechanical Event and Their Electrical and Clinical CorrelationDocument28 pagesCardiac Cycle: Mechanical Event and Their Electrical and Clinical Correlationhawas muhammed100% (1)
- Magnetic Resonance Tractographyas A Method of Choice For Neuroimaging in Ocular Ischemic Syndrome Against The Background of HypertensionDocument4 pagesMagnetic Resonance Tractographyas A Method of Choice For Neuroimaging in Ocular Ischemic Syndrome Against The Background of HypertensionCentral Asian StudiesNo ratings yet
- Format English Homework Chapter Four Cardiology Page 29-30Document3 pagesFormat English Homework Chapter Four Cardiology Page 29-30Alvi Jalilul HakimNo ratings yet
- Antihypertensive AgentsDocument39 pagesAntihypertensive AgentsFuhrer OdebsNo ratings yet
- Ecg For InternsDocument25 pagesEcg For InternszeshooNo ratings yet
- Practical Notes On Internal Medicine (TZTM)Document255 pagesPractical Notes On Internal Medicine (TZTM)Aung Zaya KyawNo ratings yet
- Approach To The Patient in Shock: by James Holencik, DODocument52 pagesApproach To The Patient in Shock: by James Holencik, DOLydia MamurNo ratings yet
- Equipment For Taking Vital SignsDocument12 pagesEquipment For Taking Vital SignsZoila EscalonaNo ratings yet
- Pharmacology Cardiovascular DrugsDocument27 pagesPharmacology Cardiovascular DrugsMitzel AlvaranNo ratings yet
- Secondary Stroke PreventionDocument54 pagesSecondary Stroke PreventionHùng Phạm Lý ChíNo ratings yet
- Lingkar Pinggang-Pinggul Dengan PJKDocument10 pagesLingkar Pinggang-Pinggul Dengan PJKDjoko SutopoNo ratings yet
- HSCRP Level-0,5Document10 pagesHSCRP Level-0,5Nova SipahutarNo ratings yet
- Vascular Technology 1000 Multiple Choice QuestionsDocument196 pagesVascular Technology 1000 Multiple Choice Questionssaimum9092% (13)
- Continuation (Altered Tissue Perfusion)Document59 pagesContinuation (Altered Tissue Perfusion)Grace Jane DionaldoNo ratings yet
- Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Document7 pagesBasic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Rizki YuliantoNo ratings yet
- 114 Final Brain Dump Part 2Document8 pages114 Final Brain Dump Part 2kelsey jacksonNo ratings yet
- Medical Surgical Lesson Plan 2 (Nursing Education)Document11 pagesMedical Surgical Lesson Plan 2 (Nursing Education)Charan100% (3)