You might also like
- Mucosal Wave Measurement Techniques for Diagnosing Voice DisordersDocument11 pagesMucosal Wave Measurement Techniques for Diagnosing Voice DisordersSRI RANJANI VNo ratings yet
- Project Yogi 3Document141 pagesProject Yogi 3Mukesh kannan MahiNo ratings yet
- Ultrasonics - Sonochemistry: SciencedirectDocument11 pagesUltrasonics - Sonochemistry: SciencedirectBreeze ChloeNo ratings yet
- Voice Rest Versus Exercise: A Review of The Literature: Madison, WisconsinDocument9 pagesVoice Rest Versus Exercise: A Review of The Literature: Madison, WisconsinJaime Crisosto AlarcónNo ratings yet
- Fresc 02 708102Document9 pagesFresc 02 708102ChawNo ratings yet
- Biological Effects of Low Frequency High IntensityDocument23 pagesBiological Effects of Low Frequency High Intensitycarolina arendNo ratings yet
- Anatomical Study of The Brachial Plexus Using SurfDocument9 pagesAnatomical Study of The Brachial Plexus Using Surfjack sparrowNo ratings yet
- Clin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsDocument7 pagesClin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsIkon ikonicNo ratings yet
- Postoperative Urinary Retention: Anesthetic and Perioperative ConsiderationsDocument19 pagesPostoperative Urinary Retention: Anesthetic and Perioperative Considerationspooria shNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- (Ajomr)Document10 pages(Ajomr)MuhasbirNo ratings yet
- Cervical AuscutationDocument18 pagesCervical AuscutationCristian Camilo HERNANDEZ PEREZNo ratings yet
- Residentes AbrilDocument3 pagesResidentes AbrilLuis Zegarra SalinasNo ratings yet
- Sulcus Vocalis Our Experience-DikonversiDocument5 pagesSulcus Vocalis Our Experience-DikonversiNuni SukindarNo ratings yet
- Vocal Function Exercises For Presbylaryn PDFDocument9 pagesVocal Function Exercises For Presbylaryn PDFAngela Lleuful ToledoNo ratings yet
- Cervical MyelpathyDocument12 pagesCervical MyelpathyannamarianeuroNo ratings yet
- Ultrasonic Topographical and Pathotopographical Anatomy: A Color AtlasFrom EverandUltrasonic Topographical and Pathotopographical Anatomy: A Color AtlasNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationDocument11 pagesA Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationRudnapon AmornlaksananonNo ratings yet
- The Utility of Pitch Elevation in the Evaluation of Oropharyngeal Dysphagia- Preliminary FindingsDocument8 pagesThe Utility of Pitch Elevation in the Evaluation of Oropharyngeal Dysphagia- Preliminary FindingsESTEFANIA GEOVANNA MEJIA MACASNo ratings yet
- Efectos Del Ultrasonido en FibroblastosDocument7 pagesEfectos Del Ultrasonido en FibroblastosErika VillacisNo ratings yet
- Full-Face Effects of Temporal Volumizing and Temporal Lifting TechniquesDocument21 pagesFull-Face Effects of Temporal Volumizing and Temporal Lifting TechniquesdubraskitaNo ratings yet
- The Sequence of Swallowing Events During The Chin-Down PostureDocument12 pagesThe Sequence of Swallowing Events During The Chin-Down PostureMarcia SantanaNo ratings yet
- Optimal Duration For Voice Rest After Vocal Fold Sugery544545454545454Document7 pagesOptimal Duration For Voice Rest After Vocal Fold Sugery544545454545454Oana MusteaţǎNo ratings yet
- Voxel-Based Lesion-Symptom Mapping: Nature Neuroscience June 2003Document4 pagesVoxel-Based Lesion-Symptom Mapping: Nature Neuroscience June 2003Gamze EşdurNo ratings yet
- MisophoniaDocument4 pagesMisophoniamsNo ratings yet
- Interpreting Diaphragmatic Movement With Bedside ImagingDocument10 pagesInterpreting Diaphragmatic Movement With Bedside ImagingSilvanaNo ratings yet
- Vocal Function Exercises For Presbylaryngis: A Multidimensional Assessment of Treatment OutcomesDocument10 pagesVocal Function Exercises For Presbylaryngis: A Multidimensional Assessment of Treatment OutcomesJulia GavrashenkoNo ratings yet
- The Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeDocument7 pagesThe Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeCentral Asian StudiesNo ratings yet
- 1 FullDocument14 pages1 FullLikhitaNo ratings yet
- Long-Term Radiologic Pulp Evaluation After Partial Pulpotomy in Young Permanent MolarsDocument9 pagesLong-Term Radiologic Pulp Evaluation After Partial Pulpotomy in Young Permanent MolarsAbdul Rahman AlmishhdanyNo ratings yet
- Orkshop On Acoustic Voice Analysis: Summary StatementDocument36 pagesOrkshop On Acoustic Voice Analysis: Summary StatementMagali MussiNo ratings yet
- Ayuse Et Al-2019-Special Care in DentistryDocument7 pagesAyuse Et Al-2019-Special Care in DentistryFrancesco TorelliNo ratings yet
- Diagnosis and Treatment of Vestibular DisordersFrom EverandDiagnosis and Treatment of Vestibular DisordersSeilesh BabuNo ratings yet
- Lou Et Al (2018) - Wound-Healing Effects of 635-nm Low-Level Laser Therapy On Primary Human Vocal Fold Epithelial Cells An in Vitro StudyDocument8 pagesLou Et Al (2018) - Wound-Healing Effects of 635-nm Low-Level Laser Therapy On Primary Human Vocal Fold Epithelial Cells An in Vitro StudyRobson LemosNo ratings yet
- Desarrollo CerebroDocument17 pagesDesarrollo CerebroBenjamin RomeroNo ratings yet
- Revised DraftDocument31 pagesRevised DraftBertrandNo ratings yet
- HHS Public Access: Ultrasound Molecular Imaging: Moving Towards Clinical TranslationDocument23 pagesHHS Public Access: Ultrasound Molecular Imaging: Moving Towards Clinical TranslationTika wahyuNo ratings yet
- JACKLER Brackmann NeurotologyDocument1,404 pagesJACKLER Brackmann NeurotologyRodrigo CabreraNo ratings yet
- (Neuromethods 150) Marco Cascella - General Anesthesia Research-Springer US - Humana (2020) PDFDocument259 pages(Neuromethods 150) Marco Cascella - General Anesthesia Research-Springer US - Humana (2020) PDFCristian C BecerraNo ratings yet
- Comparative Study Between Conventional MicrolaryngealDocument7 pagesComparative Study Between Conventional MicrolaryngealTeuku Ahmad HasanyNo ratings yet
- 2020focused Ultrasound Excites Neurons Via Mechanosensitive Calcium Accumulation and Ion Channel AmplificationDocument15 pages2020focused Ultrasound Excites Neurons Via Mechanosensitive Calcium Accumulation and Ion Channel AmplificationStress LessNo ratings yet
- Reicunaculo e MovimentoDocument11 pagesReicunaculo e MovimentoAndre GuimaraesNo ratings yet
- Vocal Fold Scars Current Concepts and Future Directions. Consensus Report of The Phonosurgery Committee of The European Laryngological SocietyDocument17 pagesVocal Fold Scars Current Concepts and Future Directions. Consensus Report of The Phonosurgery Committee of The European Laryngological Societyanitaabreu123No ratings yet
- Fluoroscopic Evaluation of Oropharyngeal Dysphagia - Anatomic, Technical, and Common Etiologic Factors - ManuscritoDocument25 pagesFluoroscopic Evaluation of Oropharyngeal Dysphagia - Anatomic, Technical, and Common Etiologic Factors - ManuscritoandrefaelNo ratings yet
- Biogenic Gas Vesicles for Ultrasound Imaging and Targeted Therapeutics (科研通-ablesci.com)Document15 pagesBiogenic Gas Vesicles for Ultrasound Imaging and Targeted Therapeutics (科研通-ablesci.com)awfultimboNo ratings yet
- Aging voice changes and treatmentsDocument5 pagesAging voice changes and treatmentsFonoaudiologiaNo ratings yet
- Human Brain Mapping - 2020 - Amoruso - Oscillatory and structural signatures of language plasticity in brain tumor patientsDocument17 pagesHuman Brain Mapping - 2020 - Amoruso - Oscillatory and structural signatures of language plasticity in brain tumor patientsAlejandro Cano VillagrasaNo ratings yet
- UntitledDocument402 pagesUntitledMilky Unique100% (1)
- 2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDocument7 pages2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDimitris RodriguezNo ratings yet
- Radiologic Assessment of The Paranasal SinusesDocument8 pagesRadiologic Assessment of The Paranasal SinusesNicolás HenaoNo ratings yet
- Avaliação Ultrassonográfica Do Músculo Genio-Hióideo e Osso Hióide Durante A Deglutição em Adultos Jovens PDFDocument6 pagesAvaliação Ultrassonográfica Do Músculo Genio-Hióideo e Osso Hióide Durante A Deglutição em Adultos Jovens PDFGiovanna MartinsNo ratings yet
- --Low-Level Laser Therapy at 635 nm for Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudyDocument5 pages--Low-Level Laser Therapy at 635 nm for Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudymarioNo ratings yet
- Focus: Focused Ultrasound-Mediated Noninvasive Blood-BrainDocument10 pagesFocus: Focused Ultrasound-Mediated Noninvasive Blood-BrainRafaelNo ratings yet
- Nihms 222369 PDFDocument18 pagesNihms 222369 PDFmariasoledaNo ratings yet
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 pagesVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123No ratings yet
- Relacion Lengua OjoDocument5 pagesRelacion Lengua OjoCamila Ignacia Diaz PaezNo ratings yet
- Speaking Without Vocal Folds Using A Machine-Learning-Assisted Wearable Sensing-Actuation SystemDocument11 pagesSpeaking Without Vocal Folds Using A Machine-Learning-Assisted Wearable Sensing-Actuation Systemphilosophos1No ratings yet
- WH Questions CuesDocument1 pageWH Questions CuesMelandes TamirisNo ratings yet
- WH Questions Cues PDFDocument6 pagesWH Questions Cues PDFMelandes TamirisNo ratings yet
- Mapping of Vocal Risk in Amateur Choir: April 2016Document12 pagesMapping of Vocal Risk in Amateur Choir: April 2016Melandes TamirisNo ratings yet
- Neurolinguis 5Document345 pagesNeurolinguis 5Melandes TamirisNo ratings yet
- Monday Tuesday Wednesday Thursday Friday Saturday Sunday: 26 November 27 28 29 30 1 December 2Document2 pagesMonday Tuesday Wednesday Thursday Friday Saturday Sunday: 26 November 27 28 29 30 1 December 2Melandes TamirisNo ratings yet
- DeVore ErDocument96 pagesDeVore ErMelandes TamirisNo ratings yet
- 12724688Document98 pages12724688Melandes Tamiris100% (1)
- G. Paul Moore LecturDocument13 pagesG. Paul Moore LecturMelandes TamirisNo ratings yet
- O Grande Debate - Dislexia BrasilDocument19 pagesO Grande Debate - Dislexia BrasilMelandes TamirisNo ratings yet
- 2009-Miellet ODonel SerenoDocument9 pages2009-Miellet ODonel SerenoMelandes TamirisNo ratings yet
- R16 IV Year Syllabus PDFDocument233 pagesR16 IV Year Syllabus PDFSai KumarNo ratings yet
- ER-56-03 EN Packager Standards Skid Design and FabricationDocument4 pagesER-56-03 EN Packager Standards Skid Design and FabricationCamilo Andres Cardozo FajardoNo ratings yet
- 49 - HD - 2000 New Logo LowDocument12 pages49 - HD - 2000 New Logo LowAgata OwczarekNo ratings yet
- Accurately Measure Mill Fill Level with Vibration-Based MillScan DSPDocument6 pagesAccurately Measure Mill Fill Level with Vibration-Based MillScan DSPmahantmtechNo ratings yet
- Free Spanning Analysis of Offshore PipelinesDocument14 pagesFree Spanning Analysis of Offshore PipelinesMaringan JuliverNo ratings yet
- IJREI - Fabrication and Analysis of Spring Testing MachineDocument6 pagesIJREI - Fabrication and Analysis of Spring Testing MachineIjrei JournalNo ratings yet
- BVP2078GBDocument10 pagesBVP2078GBRon Don jrNo ratings yet
- Concrete Crack Meter - Crack Monitoring Equipment - PCTEDocument2 pagesConcrete Crack Meter - Crack Monitoring Equipment - PCTEPrajakta RahateNo ratings yet
- Shock Absorber Design and AnalysisDocument13 pagesShock Absorber Design and AnalysisAshwini BiradarNo ratings yet
- E70-902 IB Vibration Severity Guidelines For Screw CompresorDocument4 pagesE70-902 IB Vibration Severity Guidelines For Screw CompresorBenito Antonio Formoso LouroNo ratings yet
- A Ship Motion Simulation SystemDocument11 pagesA Ship Motion Simulation SystemBENNo ratings yet
- Optimize for sound wave chapter documentDocument68 pagesOptimize for sound wave chapter documentelty TanNo ratings yet
- Technical Programme ACMFMS2012DElhiDocument19 pagesTechnical Programme ACMFMS2012DElhiSwarnava GhoshNo ratings yet
- RRRDocument31 pagesRRRddNo ratings yet
- Forced VibrationsDocument3 pagesForced VibrationsshethNo ratings yet
- The Universe Is On Your SideDocument27 pagesThe Universe Is On Your SideHélio Sr InútilNo ratings yet
- Advanced Material Removal Using Ultrasonic MachiningDocument5 pagesAdvanced Material Removal Using Ultrasonic MachiningAbhishek TuliNo ratings yet
- Chapter 7 Methods of Vibration ControlDocument75 pagesChapter 7 Methods of Vibration Controlikhleif100% (3)
- AzimaDLI Severity Chart 2013 PDFDocument1 pageAzimaDLI Severity Chart 2013 PDFEswin Paico de la CruzNo ratings yet
- Erochko Jeffrey A 201306 PHD Thesis PDFDocument470 pagesErochko Jeffrey A 201306 PHD Thesis PDFAnas IssaNo ratings yet
- M230HGE-L20 C2 Ver.2.0-6 Approval SpecificationDocument17 pagesM230HGE-L20 C2 Ver.2.0-6 Approval SpecificationpasmanteriabellaNo ratings yet
- Seismic Design: Bldg. Tech-05 - Bs Arch - 3 - OlogarDocument19 pagesSeismic Design: Bldg. Tech-05 - Bs Arch - 3 - OlogarAnonymous 5kOS4tNo ratings yet
- Heat conduction and wave equation problemsDocument32 pagesHeat conduction and wave equation problemsistopiNo ratings yet
- SDJ902Document2 pagesSDJ902B P REDDYNo ratings yet
- Determining Wind Actions Using Eurocode 1-Part 3 Worked Example - 2Document13 pagesDetermining Wind Actions Using Eurocode 1-Part 3 Worked Example - 2val mejiaNo ratings yet
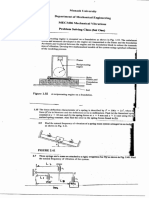
- MEC3406 Mechanical Vibrations Problem Solving Class Set OneDocument1 pageMEC3406 Mechanical Vibrations Problem Solving Class Set Onemohsin ahmedNo ratings yet
- Polish Maritime ResearchDocument32 pagesPolish Maritime ResearchparatonerqNo ratings yet
- 1 Vibration Analysis Using MATLABDocument24 pages1 Vibration Analysis Using MATLABShannon Chen TanNo ratings yet
- Husqvarna 252rxDocument48 pagesHusqvarna 252rxArijus SkarbaliusNo ratings yet
- An Introduction To Earthquake Engineering Beg 454 CiDocument2 pagesAn Introduction To Earthquake Engineering Beg 454 CiAnil MarsaniNo ratings yet