You might also like
- Machine Learning,, Mcgraw Hill, 1997.: Tom MitchellDocument1 pageMachine Learning,, Mcgraw Hill, 1997.: Tom MitchellIsaias Prestes0% (1)
- Effectofa Quality Improvement Interventionon Clinical Outcomes in Patients in India With Acute Myocardial InfarctionDocument12 pagesEffectofa Quality Improvement Interventionon Clinical Outcomes in Patients in India With Acute Myocardial InfarctionIsaias PrestesNo ratings yet
- CommunityViralLoadinHIV PDFDocument9 pagesCommunityViralLoadinHIV PDFIsaias PrestesNo ratings yet
- Type I and II ErrorsDocument2 pagesType I and II ErrorsIsaias PrestesNo ratings yet
- Installing The Hot-Spark SVDA 034 Distributor With 3BOS4U1 Electronic IgnitionDocument4 pagesInstalling The Hot-Spark SVDA 034 Distributor With 3BOS4U1 Electronic IgnitionIsaias PrestesNo ratings yet
- Installing The 009 Distributor With 3BOS4U1 Electronic IgnitionDocument6 pagesInstalling The 009 Distributor With 3BOS4U1 Electronic IgnitionIsaias PrestesNo ratings yet
- Compatible Ignition Coils, Ballast Resistors, Hot-Spark Electronic IgnitionDocument4 pagesCompatible Ignition Coils, Ballast Resistors, Hot-Spark Electronic IgnitionIsaias PrestesNo ratings yet
- How To Adjust The Idle Mixture On Holley CarbsDocument4 pagesHow To Adjust The Idle Mixture On Holley CarbsIsaias PrestesNo ratings yet
- Commercial Aircraft Design Trends and Growth ProjectionsDocument60 pagesCommercial Aircraft Design Trends and Growth ProjectionsCamelia MunteanuNo ratings yet
- How to Read a Book in 3 StagesDocument1 pageHow to Read a Book in 3 StagesAwie ClementeNo ratings yet
- Mean Separation StatisticsDocument15 pagesMean Separation StatisticsIsaias Prestes100% (1)
- Joffe Et Al Causal Diagrams in Systems EpidemiologyDocument34 pagesJoffe Et Al Causal Diagrams in Systems EpidemiologyIsaias PrestesNo ratings yet
- Lecture 13Document28 pagesLecture 13Isaias PrestesNo ratings yet
- Experimentwise Error RateDocument2 pagesExperimentwise Error RateIsaias PrestesNo ratings yet
- Fortran 90 95 Manual PDFDocument67 pagesFortran 90 95 Manual PDFsayyadmannanNo ratings yet
- 45 FullDocument2 pages45 FullIsaias PrestesNo ratings yet
- R MHWDocument189 pagesR MHWIsaias PrestesNo ratings yet
- Journal of The Brazilian Society of Mechanical Sciences and Engineering - Drag Optimization For Transport Aircraft Mission Adaptive WingDocument13 pagesJournal of The Brazilian Society of Mechanical Sciences and Engineering - Drag Optimization For Transport Aircraft Mission Adaptive WingIsaias PrestesNo ratings yet
- Decision Models For Record LinkageDocument15 pagesDecision Models For Record LinkageIsaias PrestesNo ratings yet
- FarmacocineticaDocument5 pagesFarmacocineticaIsaias PrestesNo ratings yet
- Manual Placa Mae AsusDocument72 pagesManual Placa Mae AsusLisandra SittaNo ratings yet
- STELLMAN Issues of Causality in The History of Occupational Epidemiology.Document10 pagesSTELLMAN Issues of Causality in The History of Occupational Epidemiology.Isaias PrestesNo ratings yet
- MORABIA The Making of An Epidemiological Theory of Bias and Confounding.Document1 pageMORABIA The Making of An Epidemiological Theory of Bias and Confounding.Isaias PrestesNo ratings yet
- Compaq Visual FortranDocument1,441 pagesCompaq Visual FortranIsaias PrestesNo ratings yet
- 1471 2288 6 15Document9 pages1471 2288 6 15Isaias PrestesNo ratings yet
- Doll & Hill The Mortality of Doctors in Relation To Their Smoking Habits BMJ 1954Document5 pagesDoll & Hill The Mortality of Doctors in Relation To Their Smoking Habits BMJ 1954Isaias PrestesNo ratings yet
- Ekström (2010) - On The Relation Between The Polychoric Correlation Coefficient and Spearman's Rank Correlation CoefficientDocument15 pagesEkström (2010) - On The Relation Between The Polychoric Correlation Coefficient and Spearman's Rank Correlation CoefficientIsaias PrestesNo ratings yet
- Boeing (Mcdonnell Douglas) Dc-10-30F: Aircraft VariantsDocument2 pagesBoeing (Mcdonnell Douglas) Dc-10-30F: Aircraft VariantsNadeemNo ratings yet
- Freq Leucemia Sexo QuiDocument2 pagesFreq Leucemia Sexo QuiIsaias PrestesNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- COVID-19 and Impact On Export Sector in Sri Lanka: Janaka WijayasiriDocument14 pagesCOVID-19 and Impact On Export Sector in Sri Lanka: Janaka WijayasiriShehan AnuradaNo ratings yet
- IPCC Waste ModelDocument103 pagesIPCC Waste ModelEndah Sri PraptianiNo ratings yet
- Beginner's Guide To Centrifugal Compressor Design and SimulationDocument17 pagesBeginner's Guide To Centrifugal Compressor Design and Simulationvijay_jvNo ratings yet
- Technical Guide Pigment&Coating Colour PreparationDocument18 pagesTechnical Guide Pigment&Coating Colour PreparationHuy NguyenNo ratings yet
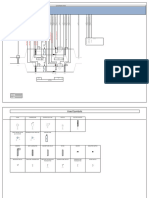
- AHU Cable Termination 2 1Document2 pagesAHU Cable Termination 2 1naing linNo ratings yet
- Sony HCD-GNX60Document76 pagesSony HCD-GNX60kalentoneschatNo ratings yet
- Bridge Bearings 2014Document167 pagesBridge Bearings 2014ErDKushwaha100% (1)
- Electrical Layout - L1Document1 pageElectrical Layout - L1sushant moreyNo ratings yet
- Roc ScienceDocument2 pagesRoc ScienceCamilo Espinoza CáceresNo ratings yet
- HSE Procedure Manual: Safety FormatsDocument20 pagesHSE Procedure Manual: Safety FormatsPavan KumarNo ratings yet
- Anodize AluminiumDocument200 pagesAnodize AluminiumYunus LorrNo ratings yet
- Equipments Used For Examination of The Female Reproductive SDocument11 pagesEquipments Used For Examination of The Female Reproductive Ssuleiman AbdullahiNo ratings yet
- Macroinvertebrates LessonDocument2 pagesMacroinvertebrates Lessonapi-497946823No ratings yet
- Company-Profile-word-final Kadakso AsiliDocument4 pagesCompany-Profile-word-final Kadakso AsiliHaron HB WritersNo ratings yet
- Free Printable Quiet BookDocument20 pagesFree Printable Quiet Bookjessarre atienzaNo ratings yet
- GMP Inspection Checklist - قائمة المراجعة (GMP)Document24 pagesGMP Inspection Checklist - قائمة المراجعة (GMP)michael_payne353280% (5)
- G10 Q1 Health Module 3Document11 pagesG10 Q1 Health Module 3Manuel Rosales Jr.No ratings yet
- Aluminium PipeDocument1 pageAluminium PipeRobin Charles SamuelNo ratings yet
- Spc42xx 43xx 52xx 53xx 63xx Installation Configuration Manual enDocument296 pagesSpc42xx 43xx 52xx 53xx 63xx Installation Configuration Manual entelecothalesNo ratings yet
- VW Transporter T5 T6 7H - Multivan 7E Multifunction Steering Wheel Retrofit Wiring HarnessDocument13 pagesVW Transporter T5 T6 7H - Multivan 7E Multifunction Steering Wheel Retrofit Wiring HarnessNull100% (1)
- The White Lotus by OSHODocument450 pagesThe White Lotus by OSHODillip Kumar MahapatraNo ratings yet
- Yank 1943jul09 PDFDocument24 pagesYank 1943jul09 PDFjohn obrienNo ratings yet
- Basic Science ParasitDocument33 pagesBasic Science ParasitNaifahLuthfiyahPutriNo ratings yet
- Dental Aesthetic and Self Confidence Among Filipino AdolescentsDocument9 pagesDental Aesthetic and Self Confidence Among Filipino Adolescentssumbu pendekNo ratings yet
- Warhammer 50k - The Shape of The Nightmare To ComeDocument115 pagesWarhammer 50k - The Shape of The Nightmare To ComeCallum MacAlister100% (1)
- Switching TrainningDocument107 pagesSwitching TrainningchinthasreenivasaraoNo ratings yet
- Assighment 3Document7 pagesAssighment 3Samih S. BarzaniNo ratings yet
- Discovering Computers 2011: Living in A Digital WorldDocument36 pagesDiscovering Computers 2011: Living in A Digital WorlddewifokNo ratings yet
- Predictive MaintenanceDocument17 pagesPredictive Maintenancejimmy_d_nasutionNo ratings yet
- 3D OBC Seismic Survey Geometry OptimizationDocument9 pages3D OBC Seismic Survey Geometry OptimizationIn SeNo ratings yet