You might also like
- SindromeDocument6 pagesSindromeAnthonyNo ratings yet
- Anaphylaxis Diagnosis and ManagementDocument10 pagesAnaphylaxis Diagnosis and Managementd dNo ratings yet
- FERRET - Evaluating and Stabilizing The Critical FerretDocument7 pagesFERRET - Evaluating and Stabilizing The Critical Ferrettaner_soysurenNo ratings yet
- Update: Seizure Management in Small Animal PracticeDocument21 pagesUpdate: Seizure Management in Small Animal Practicecatalina igorNo ratings yet
- Anaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyDocument7 pagesAnaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyFran ramos ortegaNo ratings yet
- HIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional DistalDocument3 pagesHIRSCHSPRUNG's DISEASE (Aganglionic Megacolon) Definition Presence of Large, Non-Functional Distalkhadzx100% (2)
- Feline Epilepsy Causes and TreatmentDocument13 pagesFeline Epilepsy Causes and TreatmentAleja Torres GaviriaNo ratings yet
- Neonatal SeizuresDocument6 pagesNeonatal SeizuresClaraAmeliaNo ratings yet
- Index: Acute Recurrent Ataxia Chronic Progressive Ataxia Pharmacological Management of Cerebellar DeficitsDocument31 pagesIndex: Acute Recurrent Ataxia Chronic Progressive Ataxia Pharmacological Management of Cerebellar DeficitsKhaled OssamaNo ratings yet
- Neurologic Diseases of RuminantsDocument6 pagesNeurologic Diseases of Ruminantsh8tcsfmmndNo ratings yet
- MegaesophagusDocument8 pagesMegaesophagusmar_algaNo ratings yet
- Canine Hypoadrenocorticism Pathogenesis and Clinical FeaturesDocument9 pagesCanine Hypoadrenocorticism Pathogenesis and Clinical FeaturesAna Clara SevasteNo ratings yet
- 0304_consultantoncallDocument4 pages0304_consultantoncallnessimmounir1173No ratings yet
- La Than 2018Document10 pagesLa Than 2018Alejandra QuinteroNo ratings yet
- Emergencytreatmentof Theseizuringpatient: Emergency MedicineDocument5 pagesEmergencytreatmentof Theseizuringpatient: Emergency Medicinecatalina igorNo ratings yet
- Hepatic Encephalopathy: Ammonia and Inflammation Key in HE PathogenesisDocument15 pagesHepatic Encephalopathy: Ammonia and Inflammation Key in HE PathogenesisJuan DuasoNo ratings yet
- Interpretive Summary: EosinophilsDocument2 pagesInterpretive Summary: EosinophilsIlincaNo ratings yet
- Bilateral Parotid MassDocument50 pagesBilateral Parotid MassKassim OboghenaNo ratings yet
- A Rare Cause of Pancreatic Insufficiency Johanson Blizzard SyndromeDocument3 pagesA Rare Cause of Pancreatic Insufficiency Johanson Blizzard Syndromeد نبيل عبيدNo ratings yet
- Miscellaneous Renal DiseaseDocument12 pagesMiscellaneous Renal DiseaseMusfian AgungNo ratings yet
- Brucellosis Dr. FajarDocument28 pagesBrucellosis Dr. FajarZhafran TobingNo ratings yet
- Fulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakyDocument108 pagesFulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakypadmaNo ratings yet
- Rayhel Et Al 2020 Clinicopathologic and Pathologic Characteristics of Feline Proteinuric Kidney DiseaseDocument11 pagesRayhel Et Al 2020 Clinicopathologic and Pathologic Characteristics of Feline Proteinuric Kidney DiseaseYanie Ummu ArsylaNo ratings yet
- Veterinary Neurology Symposium: Approach to Seizure PatientsDocument9 pagesVeterinary Neurology Symposium: Approach to Seizure PatientsOzkar JaraNo ratings yet
- CANINE-Idıopathic Erosive PolyarthritisDocument6 pagesCANINE-Idıopathic Erosive Polyarthritistaner_soysurenNo ratings yet
- Infantile, Childhood, and Adolescent Epilepsies.9Document34 pagesInfantile, Childhood, and Adolescent Epilepsies.9Silviana IlieNo ratings yet
- CANINE-CAnine Systemic Lupus Erythematosus - Part IDocument7 pagesCANINE-CAnine Systemic Lupus Erythematosus - Part Itaner_soysurenNo ratings yet
- RTM 5Document7 pagesRTM 5Christine Danica BiteraNo ratings yet
- Principles of Seizure ManagementDocument119 pagesPrinciples of Seizure ManagementRenan Toledo SandaloNo ratings yet
- Hiccup Due To Gastroesophageal Reflux Disease: Cem Koçkar, Mehmet İşler, Erkan Cüre, Altuğ Şenol, Abdulkadir BaştürkDocument3 pagesHiccup Due To Gastroesophageal Reflux Disease: Cem Koçkar, Mehmet İşler, Erkan Cüre, Altuğ Şenol, Abdulkadir Baştürkelisabeth stefaniNo ratings yet
- 03 X JDV NOle BGK NM UU3811655431330Document7 pages03 X JDV NOle BGK NM UU3811655431330José Alberto Valenzuela RomeroNo ratings yet
- Paediatric Nephrotic Syndrome Case ReportDocument5 pagesPaediatric Nephrotic Syndrome Case ReportAshley DayagNo ratings yet
- (KULIAH 5) Reaksi AnafilaksisDocument30 pages(KULIAH 5) Reaksi AnafilaksisArtawa Darma YudaNo ratings yet
- Chapter 23 Acquired Neuropathies PDFDocument106 pagesChapter 23 Acquired Neuropathies PDFzloncar3No ratings yet
- Group 4 1. Nallathambi, Aiswarya 2. Nagarajan, Venkateshwari 3. Narayanaswamy, Nithya 4. Nallagatla, Susmitha 5. Narra, Vindhya RaniDocument100 pagesGroup 4 1. Nallathambi, Aiswarya 2. Nagarajan, Venkateshwari 3. Narayanaswamy, Nithya 4. Nallagatla, Susmitha 5. Narra, Vindhya RaniAishwarya BharathNo ratings yet
- Ent Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanDocument86 pagesEnt Mcqs For Part I Exam: Prepared By: Dr. Fouad ShamsanAli QuwarahNo ratings yet
- Anaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006Document8 pagesAnaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006DidiNo ratings yet
- BJA 2019 - Allergic Conditions and Perioperative SettingDocument17 pagesBJA 2019 - Allergic Conditions and Perioperative SettingMILTON HALYSONNo ratings yet
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- Asfixia perinatal, compendiumDocument7 pagesAsfixia perinatal, compendiumClaudia LópezNo ratings yet
- Enfermedad GlomerularDocument7 pagesEnfermedad GlomerularKatty ZanabriaNo ratings yet
- Evaluation and Management of Status Epilepticus in ChildrenDocument13 pagesEvaluation and Management of Status Epilepticus in ChildrenAyan BiswasNo ratings yet
- LEC 03 - Pituitary TumoursDocument54 pagesLEC 03 - Pituitary TumoursIoana CozmaNo ratings yet
- Feline Hepatic Lipidosis: How I TreatDocument8 pagesFeline Hepatic Lipidosis: How I TreatDavid OliveraNo ratings yet
- Invasive Aspergillus in ELBW PrematureDocument6 pagesInvasive Aspergillus in ELBW PrematureDumitru PostolachiNo ratings yet
- Diagnosis and Management of Adrenal InsufficiencyDocument11 pagesDiagnosis and Management of Adrenal Insufficiencyinterna MANADONo ratings yet
- BOMATDocument1 pageBOMATDian NovitasariNo ratings yet
- Acr Omega LyDocument4 pagesAcr Omega LyRika PutriNo ratings yet
- Use of Toxinbinder and Immunomodulater in Treatment of Moldy Corn Poisoning in Mule's at Udayapur District, NepalDocument6 pagesUse of Toxinbinder and Immunomodulater in Treatment of Moldy Corn Poisoning in Mule's at Udayapur District, Nepalkarki Keadr DrNo ratings yet
- 0-0013 PDFDocument24 pages0-0013 PDFisabellaprie3No ratings yet
- Therapeutic Contraindications in Exotic PetsDocument14 pagesTherapeutic Contraindications in Exotic Pets黃皓No ratings yet
- Refeeding Syndrome in Small Ruminants Receiving Parenteral NutritionDocument6 pagesRefeeding Syndrome in Small Ruminants Receiving Parenteral NutritionNey TeixeiraNo ratings yet
- Cabine IsolatesDocument4 pagesCabine IsolatesbsousarobertoNo ratings yet
- 1 AEp Cut KOohnfg G7 Xga I1655431317Document10 pages1 AEp Cut KOohnfg G7 Xga I1655431317José Alberto Valenzuela RomeroNo ratings yet
- Genetic and Pediatric Diseases Chapter SummaryDocument16 pagesGenetic and Pediatric Diseases Chapter SummaryJustine HungNo ratings yet
- Metabolik EncelophatyDocument8 pagesMetabolik EncelophatyfkiaNo ratings yet
- lyle-dugas2016Document4 pageslyle-dugas2016Claudia LópezNo ratings yet
- Acute Lower Motor Neuron Tetraparesis Causes and TreatmentDocument22 pagesAcute Lower Motor Neuron Tetraparesis Causes and TreatmentWira KusumaNo ratings yet
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDocument4 pagesInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainNo ratings yet
- Simon'S Cookery Course: The Alternative Guide To Cooking - Survival or OtherwiseDocument32 pagesSimon'S Cookery Course: The Alternative Guide To Cooking - Survival or OtherwiseAengus RyanNo ratings yet
- Stigma in Access To Antiretroviral Therpy in Abuja Nigeria The Importance of Social Connections PDFDocument318 pagesStigma in Access To Antiretroviral Therpy in Abuja Nigeria The Importance of Social Connections PDFKingsley OturuNo ratings yet
- Vitamin D and The Digestive SystemDocument16 pagesVitamin D and The Digestive Systemsayangnana17No ratings yet
- Client Assessment DiagramDocument1 pageClient Assessment DiagramHeather HayenNo ratings yet
- Virology lab diagnosis methodsDocument31 pagesVirology lab diagnosis methodsjamsthemack100% (1)
- Pathogen: The Infected (Draft Copy)Document45 pagesPathogen: The Infected (Draft Copy)GnomeMadeIon100% (3)
- Neuroanatomy TractsDocument4 pagesNeuroanatomy TractsLoveHouseMDNo ratings yet
- 2012 Japanese Meridian TherapyDocument27 pages2012 Japanese Meridian Therapy1Rogerio100% (7)
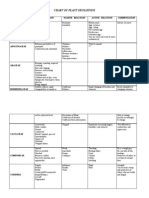
- 2.Sankaran-Chart of Plant SensationsDocument11 pages2.Sankaran-Chart of Plant Sensationsluz_188% (8)
- Lista Ingles Text Comprehension MedioDocument12 pagesLista Ingles Text Comprehension MedioDaniel SantosNo ratings yet
- Barangay Approves Funds for COVID-19 ResponseDocument2 pagesBarangay Approves Funds for COVID-19 ResponseJamy Vab MontesNo ratings yet
- God's Cancer ParmacyDocument5 pagesGod's Cancer ParmacyNick BantoloNo ratings yet
- 7 MM FrogDocument28 pages7 MM FrogNiki Reroll04No ratings yet
- Interview DrPalevskyDocument20 pagesInterview DrPalevskyzapperindiaNo ratings yet
- Body Parts Sanjeevini Healing CardsDocument24 pagesBody Parts Sanjeevini Healing CardsBala Kiran GaddamNo ratings yet
- Bb3 WHO Classification of Tumors of Haemopoietic and Lymphoid Tissues 4th 2008 PGDocument422 pagesBb3 WHO Classification of Tumors of Haemopoietic and Lymphoid Tissues 4th 2008 PGLoredana Milea Ex Lefter100% (1)
- CF2024 Elanco Parvo HDocument8 pagesCF2024 Elanco Parvo HPrakash KhangalNo ratings yet
- Borile Crystaline Bsam2b Ansci100 Laboratory Excercise1Document12 pagesBorile Crystaline Bsam2b Ansci100 Laboratory Excercise1Crystaline Ann B. BorileNo ratings yet
- Broncho-Pulmonary SegmentsDocument29 pagesBroncho-Pulmonary SegmentsArbin PanjaNo ratings yet
- Kamis, 22 APRIL 2021 Bedah Digestive Mrs/Nis/Ata: Sya/DipDocument4 pagesKamis, 22 APRIL 2021 Bedah Digestive Mrs/Nis/Ata: Sya/DipMrprads5No ratings yet
- AMYLASE TEST RESULTS AND INTERPRETATIONDocument12 pagesAMYLASE TEST RESULTS AND INTERPRETATIONsarbadev sanyalNo ratings yet
- Parathyroid GlandsDocument3 pagesParathyroid GlandsRosita RamosNo ratings yet
- Solution Manual For Generalized Linear Models 0205377939Document24 pagesSolution Manual For Generalized Linear Models 0205377939BrianGarzapeyn100% (34)
- Girl with Brain Abscess and Tetralogy of FallotDocument57 pagesGirl with Brain Abscess and Tetralogy of FallotandhikaNo ratings yet
- GGL Pelvis DelimitareDocument12 pagesGGL Pelvis DelimitareStefan AnaNo ratings yet
- Assessing The Newborn and Infant-NewDocument11 pagesAssessing The Newborn and Infant-NewJan Jamison ZuluetaNo ratings yet
- Zoology Document 2Document7 pagesZoology Document 2Donna Joanne S. Dumoran50% (2)
- Abciximab Package InsertDocument22 pagesAbciximab Package InsertbiomedjobhuntNo ratings yet
- CHDocument2 pagesCHapi-444439435No ratings yet
- DU MCA 2021 Question Paper With Answer KeyDocument10 pagesDU MCA 2021 Question Paper With Answer Keyakash debbarmaNo ratings yet