You might also like
- Photodynamic TherapyDocument5 pagesPhotodynamic TherapyPranav UpadhyayaNo ratings yet
- 2007, Vol.25, Issues 1, Photodynamic TherapyDocument114 pages2007, Vol.25, Issues 1, Photodynamic TherapyRizweta DestinNo ratings yet
- The Great Debate Over Iodine in Wound Care Continues: A Review of The LiteratureDocument14 pagesThe Great Debate Over Iodine in Wound Care Continues: A Review of The LiteratureIntan HaddadNo ratings yet
- Photodynamic Therapy - A Ray Towards PeriodonticsDocument8 pagesPhotodynamic Therapy - A Ray Towards PeriodonticsInternational Organization of Scientific Research (IOSR)No ratings yet
- Laser Photobiomodulation Over Teeth SubjectedDocument6 pagesLaser Photobiomodulation Over Teeth SubjectedJuan AndradeNo ratings yet
- L.A in Dentistry 1Document13 pagesL.A in Dentistry 1CHUKWUDI HENRYNo ratings yet
- Basic Principles of Photodynamic TherapyDocument25 pagesBasic Principles of Photodynamic TherapyĐảm PhạmNo ratings yet
- In The Name of GodDocument34 pagesIn The Name of GodFariha NormanNo ratings yet
- Photodynamic Therapy for Root CanalsDocument13 pagesPhotodynamic Therapy for Root CanalsShipra SinghNo ratings yet
- Oxidative Stress, Aging, and Diseases: Clinical Interventions in Aging DoveDocument16 pagesOxidative Stress, Aging, and Diseases: Clinical Interventions in Aging DoveMedicina EncantadaNo ratings yet
- IontophoresisDocument6 pagesIontophoresisNamrathaThalatoti ywSSAmHsULNo ratings yet
- Fordyce - Spots 2Document3 pagesFordyce - Spots 2Kartika ChandraNo ratings yet
- Local Anesthesia Review: Mechanisms, Uses, and SafetyDocument12 pagesLocal Anesthesia Review: Mechanisms, Uses, and SafetyG.S. Imanto UchihaNo ratings yet
- Lect 10 IontophoresisDocument33 pagesLect 10 IontophoresisRohan HaiderNo ratings yet
- Research Article: Received June 5, 2018 Accepted July 10, 2018 Correspondence: AjeetDocument27 pagesResearch Article: Received June 5, 2018 Accepted July 10, 2018 Correspondence: AjeetajeetNo ratings yet
- Low Level Laser Therapy in Periodontics  "A ReviewDocument5 pagesLow Level Laser Therapy in Periodontics  "A ReviewIJAR JOURNALNo ratings yet
- Endodontic DisesaeDocument9 pagesEndodontic DisesaeNouman NoorNo ratings yet
- Deoliveira2014 PDT PDFDocument7 pagesDeoliveira2014 PDT PDFShriya ShahuNo ratings yet
- Occupational and EnvironmentalDocument117 pagesOccupational and EnvironmentalGideon K. MutaiNo ratings yet
- The New Oxygen Prescription: The Miracle of Oxidative TherapiesFrom EverandThe New Oxygen Prescription: The Miracle of Oxidative TherapiesRating: 5 out of 5 stars5/5 (16)
- Orally Active Multi-Functional Antioxidants Are Neuroprotective in A Rat Model of Light-Induced Retinal DamageDocument13 pagesOrally Active Multi-Functional Antioxidants Are Neuroprotective in A Rat Model of Light-Induced Retinal Damagejrandaz12No ratings yet
- Coupled Blue and Red Light-Emitting Diodes Therapy Efficacy in Patients With Rosacea Two Case Reports.Document5 pagesCoupled Blue and Red Light-Emitting Diodes Therapy Efficacy in Patients With Rosacea Two Case Reports.Carolina Hoch FariasNo ratings yet
- SOD Expert Review PDFDocument11 pagesSOD Expert Review PDFMuhammad Bayu Zohari Hutagalung100% (1)
- Dissertation LeucodermaDocument90 pagesDissertation LeucodermaRashmi Mishra100% (1)
- Cleaning SeminarDocument32 pagesCleaning Seminaresraa adelNo ratings yet
- Marine Biotoxins Origins, Effects, Distribution, Prevention and TreatmentDocument14 pagesMarine Biotoxins Origins, Effects, Distribution, Prevention and TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Artigo LED RosaceaDocument5 pagesArtigo LED RosaceaAlba SouzaNo ratings yet
- Zinc Overview PDFDocument11 pagesZinc Overview PDFLê Nguyễn Hoàng Anh100% (1)
- Cardiovasc Drugs Ther Nitrates 2011Document16 pagesCardiovasc Drugs Ther Nitrates 2011Darian HerascuNo ratings yet
- Corticosteriods Part ViiDocument8 pagesCorticosteriods Part ViiVikas VikiNo ratings yet
- International Journal of Infectious DiseasesDocument5 pagesInternational Journal of Infectious Diseasesduverney.gaviriaNo ratings yet
- Basics of Contrast Media PDFDocument1 pageBasics of Contrast Media PDFLorenaSouzaSantosNo ratings yet
- Oral Minoxidil 2023Document10 pagesOral Minoxidil 2023maat1No ratings yet
- Oral minoxidil treatment for hair loss- REVIEW JAADDocument10 pagesOral minoxidil treatment for hair loss- REVIEW JAADAndrés WunderwaldNo ratings yet
- Antioxidants (MBBS Lecture)Document76 pagesAntioxidants (MBBS Lecture)Seema VaswaniNo ratings yet
- Advances in Laser Technology and Cold Lasers in Periodontal Therapy A Review PDFDocument4 pagesAdvances in Laser Technology and Cold Lasers in Periodontal Therapy A Review PDFInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Antioxidant and AntiInflammatory Effects of Shungite Against Ultraviolet B IrradiationInduced Skin DamageDocument12 pagesAntioxidant and AntiInflammatory Effects of Shungite Against Ultraviolet B IrradiationInduced Skin DamageMatthew KleeNo ratings yet
- Walia 2000Document2 pagesWalia 2000RedwineshandyNo ratings yet
- Enhancement of Transdermal Drug Penetration by IontophoresisDocument19 pagesEnhancement of Transdermal Drug Penetration by Iontophoresisharsh raizadaNo ratings yet
- PDF 27feb24 0948 SplittedDocument4 pagesPDF 27feb24 0948 Splittedks7580713No ratings yet
- UseofNicotinamideindermatology PDFDocument9 pagesUseofNicotinamideindermatology PDFAmiraNo ratings yet
- 10th Science Important Questions & AnswersDocument4 pages10th Science Important Questions & AnswersLAKSHMI BNo ratings yet
- Actinic Cheratosis - A ReviewDocument4 pagesActinic Cheratosis - A ReviewMARIUS-MIRCEA POPESCU-MICLOSANUNo ratings yet
- Study On The Role of Gold Nanoparticles On External Beam Radiation Using Fricke GelDocument6 pagesStudy On The Role of Gold Nanoparticles On External Beam Radiation Using Fricke GelInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nutri TherapyDocument2 pagesNutri TherapySamuel DiazNo ratings yet
- Toxics 11 00555Document19 pagesToxics 11 00555linaldi1No ratings yet
- Organophosphate Poisoning Case ScenarioDocument50 pagesOrganophosphate Poisoning Case ScenarioArun NairNo ratings yet
- Group 5 - Pathogenesis of ErythrodermaDocument20 pagesGroup 5 - Pathogenesis of Erythrodermaachmad billy hakiemNo ratings yet
- Photodynamic Therapy in Endodontics: ReviewDocument15 pagesPhotodynamic Therapy in Endodontics: ReviewFabro HMNo ratings yet
- Reactive Oxygen Species Along With Reactive Nitrogen Species (ROS/RNS) As The Main Cause of Multiple SclerosisDocument15 pagesReactive Oxygen Species Along With Reactive Nitrogen Species (ROS/RNS) As The Main Cause of Multiple SclerosisSomayeh ZaminpiraNo ratings yet
- Infrared Light Therapy White PaperDocument13 pagesInfrared Light Therapy White PaperHO Andjeli100% (1)
- Fordyce Spots 3Document3 pagesFordyce Spots 3Kartika ChandraNo ratings yet
- Molecular Mechanism of Fluoride Induced Oxidative Stress and Its Possible Reversal by Chelation TherapyDocument27 pagesMolecular Mechanism of Fluoride Induced Oxidative Stress and Its Possible Reversal by Chelation TherapyAshitosh KumarNo ratings yet
- EE3018 Literature ReportDocument10 pagesEE3018 Literature ReportGoh Cai YuNo ratings yet
- Stings - Scorpion and SnakeDocument3 pagesStings - Scorpion and Snakenirmala pahadiNo ratings yet
- International Journal of SurgeryDocument5 pagesInternational Journal of SurgeryinoesienaNo ratings yet
- Risk Management Related To The Presence of Lead in Drinking Water: A Literature ReviewDocument5 pagesRisk Management Related To The Presence of Lead in Drinking Water: A Literature ReviewIJAR JOURNALNo ratings yet
- Classification and Uses of Common AntisepticsDocument34 pagesClassification and Uses of Common AntisepticsNoreak SokNo ratings yet
- Trivedi Effect - Spectroscopic Characterization of Disodium Hydrogen Orthophosphate and Sodium Nitrate After Biofield TreatmentDocument5 pagesTrivedi Effect - Spectroscopic Characterization of Disodium Hydrogen Orthophosphate and Sodium Nitrate After Biofield TreatmentTrivedi EffectNo ratings yet
- Khurana2019 PDFDocument9 pagesKhurana2019 PDFEka FaridaNo ratings yet
- Is Matter Around Us PureDocument188 pagesIs Matter Around Us Puresasi.curieNo ratings yet
- Indiabix MicrobiologyDocument47 pagesIndiabix MicrobiologyZllison Mae Teodoro MangabatNo ratings yet
- Bio 110 - Chapter 5Document32 pagesBio 110 - Chapter 5moayadNo ratings yet
- Prausnitz Derm Book Chapter 2012Document10 pagesPrausnitz Derm Book Chapter 2012Valentina AdindaNo ratings yet
- Beetroot Permeability With TemperatureDocument8 pagesBeetroot Permeability With TemperatureAlex BoumanNo ratings yet
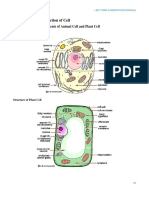
- Cells: The Basics: Cytoplasm. Protein-Making Bodies Called Ribosomes Also Form Part of The Cytoplasm. Like AllDocument4 pagesCells: The Basics: Cytoplasm. Protein-Making Bodies Called Ribosomes Also Form Part of The Cytoplasm. Like AllJanelyn GarinNo ratings yet
- Exam ReviewDocument12 pagesExam Reviewmadison.cosbyNo ratings yet
- B 28050253Document546 pagesB 28050253Madalina HerNo ratings yet
- Frantisek Baluska Plant-Environment InteractionsBookFi - OrgDocument313 pagesFrantisek Baluska Plant-Environment InteractionsBookFi - OrgsuhartiniNo ratings yet
- Murray: Medical Microbiology, 6 Edition: Chapter 02: Bacterial Classification, Structure, and Replication Test BankDocument3 pagesMurray: Medical Microbiology, 6 Edition: Chapter 02: Bacterial Classification, Structure, and Replication Test Bankاحمد كرمNo ratings yet
- Cell Structure Gizmo AnswersDocument5 pagesCell Structure Gizmo Answerspaula-navas 13451No ratings yet
- Post Basic B SC 1st YearDocument3 pagesPost Basic B SC 1st Yearvijaykadam_nda67% (3)
- As Biology SampleDocument42 pagesAs Biology Samplelucylovesbooks6770No ratings yet
- Application of Tethered Bilayers For Detection of Bacterial ToxinsDocument31 pagesApplication of Tethered Bilayers For Detection of Bacterial ToxinsGintaras ValinciusNo ratings yet
- Cell CrosswordDocument2 pagesCell CrosswordLycanAlfaNo ratings yet
- STC 222-1Document106 pagesSTC 222-1Edeh Joshua100% (1)
- Prescotts Microbiology 10th Edition Willey Solutions Manual 1Document4 pagesPrescotts Microbiology 10th Edition Willey Solutions Manual 1ruth98% (47)
- Effect of Temperatures On The Permeability of Beetroot Cell Membranes in LatviaDocument16 pagesEffect of Temperatures On The Permeability of Beetroot Cell Membranes in LatviaMariam Al.hellaniNo ratings yet
- Lesson 2 - Prokaryotic CellsDocument2 pagesLesson 2 - Prokaryotic CellsKerberos DelabosNo ratings yet
- The Fluid Mosaic Model: Phospholipid BilayerDocument3 pagesThe Fluid Mosaic Model: Phospholipid BilayerSmarika NiraulaNo ratings yet
- Test Bank For Biochemistry A Short Course 2nd Edition John L Tymoczko Isbn 10 1429283602 Isbn 13 9781429283601Document13 pagesTest Bank For Biochemistry A Short Course 2nd Edition John L Tymoczko Isbn 10 1429283602 Isbn 13 9781429283601Angela Roberts100% (36)
- Amino Acids, Peptides & Proteins Structures and FunctionsDocument117 pagesAmino Acids, Peptides & Proteins Structures and FunctionsdharshiiniNo ratings yet
- Membran SelDocument62 pagesMembran SelLena EnjelinaNo ratings yet
- Make and Test Polysulfone MembraneDocument9 pagesMake and Test Polysulfone MembraneRizki AuNo ratings yet
- 083 41 Final Biologi T4 DLP-30-60Document31 pages083 41 Final Biologi T4 DLP-30-60Farhan DarwisyNo ratings yet
- OCR A Level Biology Content Year 1 Checklist 2015Document8 pagesOCR A Level Biology Content Year 1 Checklist 2015willNo ratings yet
- General Biology 1 Lab: Modules 1 To 3Document22 pagesGeneral Biology 1 Lab: Modules 1 To 3Naomi BelonioNo ratings yet
- 6.1 Digestion AbsorptionDocument51 pages6.1 Digestion AbsorptionormattNo ratings yet
- DNA Extraction OverviewDocument14 pagesDNA Extraction OverviewNicholas SoNo ratings yet
- Week 4 - Cell Organelles and FunctionDocument43 pagesWeek 4 - Cell Organelles and FunctionDesiree Pescasio DimasuayNo ratings yet