You might also like
- Cat Behaviour GuideDocument20 pagesCat Behaviour Guideredlandadam100% (2)
- Ebook Elitefts Ptw42Document204 pagesEbook Elitefts Ptw42Richard Marcus Seigel100% (7)
- Instant Pot Jambalaya (SO Easy!) : IngredientsDocument2 pagesInstant Pot Jambalaya (SO Easy!) : IngredientsGrace Pastorfide-AritaoNo ratings yet
- Eating To Win PDFDocument102 pagesEating To Win PDFDen KongNo ratings yet
- Allrecipes 2018Document104 pagesAllrecipes 2018Christian Del Barco67% (3)
- Buff Dudes Bulking Book Free EditionDocument16 pagesBuff Dudes Bulking Book Free EditionEric Tan88% (8)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- DHARMA Mac & Cheese SupperDocument1 pageDHARMA Mac & Cheese SupperRenan MasNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Acceptability of White Taro (Colocasia Esculena) JamDocument19 pagesAcceptability of White Taro (Colocasia Esculena) JamArcy CrizaldoNo ratings yet
- 5 Components of Fitness/Exercise Plan/FITT PowerpointDocument26 pages5 Components of Fitness/Exercise Plan/FITT Powerpointdnorton5437100% (7)
- Consumer Behavior Assignment (Updated)Document10 pagesConsumer Behavior Assignment (Updated)Goh Koon LoongNo ratings yet
- Paper Title: (16 Bold Blue Color)Document9 pagesPaper Title: (16 Bold Blue Color)Fauzi RusdiantoNo ratings yet
- Paper Title: (16 Bold)Document9 pagesPaper Title: (16 Bold)stretty13No ratings yet
- Paper TemplateDocument9 pagesPaper Templateadham ahmedNo ratings yet
- Paper TemplateDocument10 pagesPaper Templatenur hidayatNo ratings yet
- Stellar CrestorDocument9 pagesStellar CrestorMarwan NasriNo ratings yet
- Study of Plasma Level of Atorvastatin and Its Effect On Lipid ProfileDocument10 pagesStudy of Plasma Level of Atorvastatin and Its Effect On Lipid Profileheema valeraNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- Low-Dose Rosuvastatin Improves Lipids in Type 2 DiabetesDocument11 pagesLow-Dose Rosuvastatin Improves Lipids in Type 2 DiabetesZahid MahmoodNo ratings yet
- Clinical research shows rosuvastatin more effective than atorvastatin for metabolic syndromeDocument9 pagesClinical research shows rosuvastatin more effective than atorvastatin for metabolic syndromeSohail AhmedNo ratings yet
- j3 2010Document12 pagesj3 2010Taha FransNo ratings yet
- Effects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenDocument8 pagesEffects of Diet and Simvastatin On Serum Lipids, Insulin, and Antioxidants in Hypercholesterolemic MenAranel BomNo ratings yet
- Effects of Cinacalcet on CV Risk, Fractures & QoL in SHPTDocument8 pagesEffects of Cinacalcet on CV Risk, Fractures & QoL in SHPTannarchyNo ratings yet
- Do Angiotensin Converting Enzyme Inhibitors or Angiotensin Receptor Blockers Prevent Diabetes Mellitus? A Meta-AnalysisDocument9 pagesDo Angiotensin Converting Enzyme Inhibitors or Angiotensin Receptor Blockers Prevent Diabetes Mellitus? A Meta-AnalysisURSULA LAZONo ratings yet
- Ator Simvas OkDocument7 pagesAtor Simvas OkGatiNo ratings yet
- Evaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsDocument5 pagesEvaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsfiqaalkasieNo ratings yet
- Accepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDocument14 pagesAccepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDianne GalangNo ratings yet
- NursingresearchreportDocument12 pagesNursingresearchreportapi-300699057No ratings yet
- Hari 2018Document11 pagesHari 2018rahmansetiawanajaNo ratings yet
- Comparison of The Efficacy of Rosuvastatin Versus Atorvastatin, Simvastatin, and Pravastatin in Achieving Lipid Goals: Results From The STELLAR TrialDocument11 pagesComparison of The Efficacy of Rosuvastatin Versus Atorvastatin, Simvastatin, and Pravastatin in Achieving Lipid Goals: Results From The STELLAR Trialamit khanNo ratings yet
- Original Research: Clinical Therapeutics/Volume 40, Number 2, 2018Document20 pagesOriginal Research: Clinical Therapeutics/Volume 40, Number 2, 2018Annisa Purnama NingsihNo ratings yet
- BMC Family PracticeDocument19 pagesBMC Family PracticeFirda AndiNo ratings yet
- The Association Between Nonalcoholic Fatty Liver Disease and Stroke: Results From The Korean Genome and Epidemiology Study (Koges)Document11 pagesThe Association Between Nonalcoholic Fatty Liver Disease and Stroke: Results From The Korean Genome and Epidemiology Study (Koges)winnerfromparisNo ratings yet
- Dia Care-2006-Knopp-1478-85Document8 pagesDia Care-2006-Knopp-1478-85Barbara Sakura RiawanNo ratings yet
- Intraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseDocument6 pagesIntraplatelet Serotonin in Patients With Diabetes Mellitus and Peripheral Vascular DiseaseHyeon DaNo ratings yet
- To Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFDocument7 pagesTo Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFJez RarangNo ratings yet
- Nursing Research PresentaionDocument33 pagesNursing Research Presentaionapi-300699057No ratings yet
- STELLARmanuscriptDocument17 pagesSTELLARmanuscriptperjadanutNo ratings yet
- Order - 523187 - Main Document With Abstract - TRACKED - REVISEDDocument12 pagesOrder - 523187 - Main Document With Abstract - TRACKED - REVISEDAn MNo ratings yet
- Ezetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneDocument9 pagesEzetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneEditor ERWEJNo ratings yet
- Objective:: BackgroundDocument23 pagesObjective:: BackgroundJanine DimaangayNo ratings yet
- Milaaaaaaa FDocument12 pagesMilaaaaaaa F200742 Elya AmaliaNo ratings yet
- Comparative Study of Atorvastatin and RosuvastatinDocument8 pagesComparative Study of Atorvastatin and RosuvastatinDewi nur thohidahNo ratings yet
- A Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromeDocument7 pagesA Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromegiannidietNo ratings yet
- Metabolic cardiovascular disease risk factors and their clustering in subclinical hypothyroidismDocument7 pagesMetabolic cardiovascular disease risk factors and their clustering in subclinical hypothyroidismMaria Alice BourneufNo ratings yet
- Alhamdulillah Ada JurnalnyaDocument6 pagesAlhamdulillah Ada JurnalnyaNovriman LiviaNo ratings yet
- HOMA Medicion EJIM2003Document6 pagesHOMA Medicion EJIM2003Dr Dart05No ratings yet
- Association Between Protein Intake and Mortality in Hypertensive Patients Without Chronic Kidney Disease in The OLD-HTA CohortDocument14 pagesAssociation Between Protein Intake and Mortality in Hypertensive Patients Without Chronic Kidney Disease in The OLD-HTA Cohortluis Gomez VallejoNo ratings yet
- Antioxidant Effects of Zinc Supplementation in Tunisians With Type 2 Diabetes MellitusDocument6 pagesAntioxidant Effects of Zinc Supplementation in Tunisians With Type 2 Diabetes MellitusgautomsahariaNo ratings yet
- Effects On Serum Uric Acid by Difference of The Renal Protective Effects With Atorvastatin and Rosuvastatin in Chronic Kidney Disease PatientsDocument6 pagesEffects On Serum Uric Acid by Difference of The Renal Protective Effects With Atorvastatin and Rosuvastatin in Chronic Kidney Disease PatientsAnonymous ZbhBxeEVNo ratings yet
- Effects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesDocument12 pagesEffects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesLutfi MalefoNo ratings yet
- The Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsDocument9 pagesThe Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsLucky PratamaNo ratings yet
- Fastfood - HITDocument8 pagesFastfood - HITCarl D'heerNo ratings yet
- Sulodexide For Kidney Protection in Type 2 Diabetes PatientsDocument8 pagesSulodexide For Kidney Protection in Type 2 Diabetes PatientsFerdinand YuzonNo ratings yet
- High Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaDocument7 pagesHigh Risk of Coagulopathy Among Type-2 Diabetes Mellitus Clients at A Municipal Hospital in GhanaLovi AnaNo ratings yet
- Clinical Trial 2016Document11 pagesClinical Trial 2016guugle gogleNo ratings yet
- Paper Insulin Resistance and Ferritin As Major Determinants of Nonalcoholic Fatty Liver Disease in Apparently Healthy Obese PatientsDocument7 pagesPaper Insulin Resistance and Ferritin As Major Determinants of Nonalcoholic Fatty Liver Disease in Apparently Healthy Obese PatientsNike Dwi Putri LestariNo ratings yet
- Hypertension Management Algorithm For Type 2 Diabetic Patients Applied in Primary CareDocument5 pagesHypertension Management Algorithm For Type 2 Diabetic Patients Applied in Primary CareMarco Free-MindNo ratings yet
- Tolvaptan PDFDocument8 pagesTolvaptan PDFDaniel Rico FuentesNo ratings yet
- HypertensionDocument7 pagesHypertensionrohayatjohnNo ratings yet
- IOSR Journal of Pharmacy (IOSRPHR)Document6 pagesIOSR Journal of Pharmacy (IOSRPHR)IOSR Journal of PharmacyNo ratings yet
- Cud BdiabetesDocument10 pagesCud BdiabetesShitanjni WatiNo ratings yet
- Stratified Treatment of HypertensionDocument7 pagesStratified Treatment of HypertensionMohamad MuntahaNo ratings yet
- Randomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusDocument4 pagesRandomized Controlled Trial of Tinospora Crispa For Additional Therapy in Patients With Type 2 Diabetes MellitusEva SuryantiNo ratings yet
- Nutrients 08 00073Document9 pagesNutrients 08 00073Irma RakhmawatiNo ratings yet
- Effect of Candesartan Monotherapy On Lipid Metabolism in Patients With Hypertension: A Retrospective Longitudinal Survey Using Data From Electronic Medical RecordsDocument7 pagesEffect of Candesartan Monotherapy On Lipid Metabolism in Patients With Hypertension: A Retrospective Longitudinal Survey Using Data From Electronic Medical RecordsAldiKurosakiNo ratings yet
- Dietary protein restriction improves outcomes in diabetic nephropathyDocument9 pagesDietary protein restriction improves outcomes in diabetic nephropathyJose J.No ratings yet
- Compaison of SgotDocument4 pagesCompaison of SgotPournima WaghmareNo ratings yet
- 1519 FullDocument6 pages1519 Fullpharmas1114No ratings yet
- Biochemical Changes Associated With The Processing of FoodsDocument4 pagesBiochemical Changes Associated With The Processing of FoodsAdapa Prabhakara GandhiNo ratings yet
- Remaja - Skripsi. Universitas Sumatera Utara.: Daftar PustakaDocument5 pagesRemaja - Skripsi. Universitas Sumatera Utara.: Daftar PustakaimNo ratings yet
- Icjpir-15-103 9-14Document6 pagesIcjpir-15-103 9-14Sriram NagarajanNo ratings yet
- Taller de Ingles Tercer PeriodoDocument10 pagesTaller de Ingles Tercer PeriodoalexandrasNo ratings yet
- History of MilletsDocument4 pagesHistory of Milletsshawana rajpootNo ratings yet
- Seminar Non-ThesisDocument52 pagesSeminar Non-ThesisUmar Sabo BabaNo ratings yet
- Simvastatin (Simvador, Zocor)Document4 pagesSimvastatin (Simvador, Zocor)Riri MonicaNo ratings yet
- Herpes Virus Is The Most Common Opportunistic Infection Causing Genital Lesion in HIV PatientsDocument20 pagesHerpes Virus Is The Most Common Opportunistic Infection Causing Genital Lesion in HIV PatientsRichaNo ratings yet
- Innovation and progress at Searl Technology Ltd headquarters in GlasgowDocument50 pagesInnovation and progress at Searl Technology Ltd headquarters in GlasgowSamuel KinsNo ratings yet
- Honey and Cinnamon: A Mixture For CuresDocument23 pagesHoney and Cinnamon: A Mixture For CurescheshankarNo ratings yet
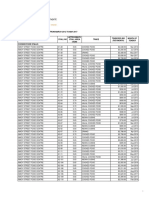
- Tender Bids From March 2012 To April 2017Document62 pagesTender Bids From March 2012 To April 2017scribd_109097762No ratings yet
- Non-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaDocument11 pagesNon-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaPatrícia Felix ÁvilaNo ratings yet
- Fasting of Persons With Diabetes Mellitus During RamadanDocument10 pagesFasting of Persons With Diabetes Mellitus During RamadanlaymenadrNo ratings yet
- Nutrition and Vascular DementiaDocument6 pagesNutrition and Vascular Dementiaapi-150223943No ratings yet
- Contents WajaDocument5 pagesContents WajaAnonymous WPCglsJl7SNo ratings yet
- The Greatest Thing Since Sliced Bread A Review of The Benefits of Processed Foods. EUFIC REVIEW. The European Food Information Council.Document6 pagesThe Greatest Thing Since Sliced Bread A Review of The Benefits of Processed Foods. EUFIC REVIEW. The European Food Information Council.Amanda Carolina Mistruzzi SanábioNo ratings yet
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapyShelly Dwi SilvitaNo ratings yet
- Ampalaya As Nutritious BiscuitDocument1 pageAmpalaya As Nutritious BiscuitAnonymous DFO1OEwuTONo ratings yet
- Nutrition and Menopause ReferencesDocument2 pagesNutrition and Menopause ReferencesNumbi HerizasiwiNo ratings yet
- Oxidation in Omega-3 Oils: An OverviewDocument8 pagesOxidation in Omega-3 Oils: An Overviewjorge alberto regalado arcayaNo ratings yet