You might also like
- IdentifyinggapsDocument6 pagesIdentifyinggapsapi-426094285No ratings yet
- Expert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancerDocument10 pagesExpert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancermarrajoanaNo ratings yet
- Long-Term Cosmesis Following A Novel Schedule ofDocument7 pagesLong-Term Cosmesis Following A Novel Schedule ofEmin PehlivanogluNo ratings yet
- NRG Consensus Contouring Guidelines For Postop emCA + CervixDocument12 pagesNRG Consensus Contouring Guidelines For Postop emCA + Cervixgermanfutbol7No ratings yet
- Elective Clinical Target Volumes For Conformal Therapy in Anorectal Cancer - An Radiation Therapy Oncology Group Consensus Panel Contouring AtlasDocument7 pagesElective Clinical Target Volumes For Conformal Therapy in Anorectal Cancer - An Radiation Therapy Oncology Group Consensus Panel Contouring AtlasAnonymous 8KN8IR1GTWNo ratings yet
- Escamoso de Esofago Cervical Metaanalisis, Guler 2022Document2 pagesEscamoso de Esofago Cervical Metaanalisis, Guler 2022Carlos N. Rojas PuyolNo ratings yet
- International Journal of Radiation Oncology Biology Physics evaluates consensus contours for CT vs MRI in brachytherapyDocument1 pageInternational Journal of Radiation Oncology Biology Physics evaluates consensus contours for CT vs MRI in brachytherapythereberryNo ratings yet
- Baumann 2016 IJROBP Development Validation of Bladder Contouring AtlasDocument9 pagesBaumann 2016 IJROBP Development Validation of Bladder Contouring AtlaszanNo ratings yet
- Beriwal Et Al 2006 Comparison of 2d Vs 3d Dosimetry For Rotte y Applicator High Dose Rate Brachytherapy For MedicallyDocument7 pagesBeriwal Et Al 2006 Comparison of 2d Vs 3d Dosimetry For Rotte y Applicator High Dose Rate Brachytherapy For MedicallyMilda InayahNo ratings yet
- Literature Review With PGI Guidelines For Delineation of Clinical Target Volume For Intact Carcinoma CervixDocument9 pagesLiterature Review With PGI Guidelines For Delineation of Clinical Target Volume For Intact Carcinoma CervixThiraviyam MbbsNo ratings yet
- s13027 020 00299 3Document10 pagess13027 020 00299 3Remona RemoraNo ratings yet
- Cancer Science - 2022 - Liu - A Bayesian Network Predicting Survival of Cervical Cancer Patients Based On SurveillanceDocument11 pagesCancer Science - 2022 - Liu - A Bayesian Network Predicting Survival of Cervical Cancer Patients Based On SurveillanceRony TeguhNo ratings yet
- Appl Physiol Nutr MetabDocument10 pagesAppl Physiol Nutr MetabAna Leticia RibeiroNo ratings yet
- Consensus Guideline On Breast Cancer Lumpectomy MarginsDocument6 pagesConsensus Guideline On Breast Cancer Lumpectomy MarginsSubhamSarthakNo ratings yet
- Ditkofsky 2015Document28 pagesDitkofsky 2015Allython Jureth Peña ReyesNo ratings yet
- Challenges in Management of Squamous Cell Carcinoma of The Anus in New England and Across The United StatesDocument5 pagesChallenges in Management of Squamous Cell Carcinoma of The Anus in New England and Across The United StatesNasrudin EfendiNo ratings yet
- 10 1111@codi 15424Document22 pages10 1111@codi 15424yongky sugandaNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- Detection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009Document8 pagesDetection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009samouille6666No ratings yet
- ESTRO-ACROPDocument12 pagesESTRO-ACROPAndreyson SilvaNo ratings yet
- Artikel MBT Flowrate DCEMRIDocument9 pagesArtikel MBT Flowrate DCEMRILucas ParretNo ratings yet
- Skin Cancer!Document8 pagesSkin Cancer!HudiansyahNo ratings yet
- Internal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionDocument3 pagesInternal Mammary Node Irradiation in Breast Cancer: The Issue of Patient SelectionmarrajoanaNo ratings yet
- Berger 2007Document9 pagesBerger 2007Benfredj KhalilNo ratings yet
- T 202200883Document7 pagesT 202200883i'm KaiyNo ratings yet
- KJR 22 1172Document13 pagesKJR 22 1172Marjorie Elizabeth Ovalle ValdesNo ratings yet
- PancreatitisDocument13 pagesPancreatitissebas2008No ratings yet
- Effective Dose of Dental CBCT LudlowDocument25 pagesEffective Dose of Dental CBCT LudlowMaríaPazSalinasVillagraNo ratings yet
- 2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsDocument1 page2011 - Kim, Kim, Beriwal - Contouring Inguinal and Femoral Nodes How Much Margin Is Needed Around The VesselsPoljarLijanNo ratings yet
- European Journal of Surgical OncologyDocument7 pagesEuropean Journal of Surgical OncologyElisa LeonteNo ratings yet
- EBM2Document8 pagesEBM2ica ssNo ratings yet
- Role of MRI in The Staging of Breast Cancer Patients: Does Histological Type and Molecular Subtype Matter?Document6 pagesRole of MRI in The Staging of Breast Cancer Patients: Does Histological Type and Molecular Subtype Matter?Ther RayNo ratings yet
- Association Between Trimester and Outcomes After Cholecystectomy During PregnancyDocument9 pagesAssociation Between Trimester and Outcomes After Cholecystectomy During PregnancyElías MendezNo ratings yet
- Geographical Distribution of Breast Cancers On The Mammogram: An Interval Cancer DatabaseDocument6 pagesGeographical Distribution of Breast Cancers On The Mammogram: An Interval Cancer DatabaseTher RayNo ratings yet
- 1 s2.0 S174868151730181X MainDocument9 pages1 s2.0 S174868151730181X MainChiara BoccalettoNo ratings yet
- Atm 07 14 323Document9 pagesAtm 07 14 323Ethel GeanNo ratings yet
- Fonc 13 1162683Document2 pagesFonc 13 1162683vinadata01No ratings yet
- Pancreatic Duct TextureDocument9 pagesPancreatic Duct TextureAdarsh GhoshNo ratings yet
- Recomendaciones PatologiaDocument10 pagesRecomendaciones PatologiahenryNo ratings yet
- Role of Lymphadenectomy During Radical CystectomyDocument8 pagesRole of Lymphadenectomy During Radical CystectomyadolfoNo ratings yet
- Bladder distension reduces OAR dose in cervical brachytherapyDocument5 pagesBladder distension reduces OAR dose in cervical brachytherapyMourya AnkurNo ratings yet
- Comparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Document5 pagesComparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Michelle LEINo ratings yet
- P1 Functional Outcomes and Health-Related QualityDocument11 pagesP1 Functional Outcomes and Health-Related Qualityernitaranterupang79No ratings yet
- Sensor WorkingDocument17 pagesSensor WorkingEngr Kashi YousafzaiNo ratings yet
- bcr2692Document16 pagesbcr2692Me KhNo ratings yet
- Outcomes Following Surgery For Colorectal Live 2016 International Journal ofDocument1 pageOutcomes Following Surgery For Colorectal Live 2016 International Journal ofoomculunNo ratings yet
- Comprehensive Ultrasound Diagnosis For Intraductal Spread of Primary Breast CancerDocument10 pagesComprehensive Ultrasound Diagnosis For Intraductal Spread of Primary Breast CancerferdiNo ratings yet
- Contrast-Enhanced MammographyFrom EverandContrast-Enhanced MammographyMarc LobbesNo ratings yet
- Final CapstoneDocument11 pagesFinal Capstoneapi-603721790No ratings yet
- Xu 2021Document9 pagesXu 2021Drsaumyta MishraNo ratings yet
- Multiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiDocument10 pagesMultiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiRicardo MirandaNo ratings yet
- Computed Tomography ColonographyDocument6 pagesComputed Tomography ColonographyC JoanesNo ratings yet
- Capstone Paper Section III Group6 1Document12 pagesCapstone Paper Section III Group6 1api-543045416No ratings yet
- Recist 1Document11 pagesRecist 1Kelik WagiyantoNo ratings yet
- Does Obesity Impact Lymph Node Retrieval in Colon CancerDocument5 pagesDoes Obesity Impact Lymph Node Retrieval in Colon Cancersee yinNo ratings yet
- BJR 20210389Document10 pagesBJR 20210389Camilo SotomayorNo ratings yet
- Comparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldDocument8 pagesComparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldAmalia fhyNo ratings yet
- 1 s2.0 S2405457723000517 MainDocument10 pages1 s2.0 S2405457723000517 Mainozlemyilmaz1820No ratings yet
- González-Correa 2019 J. Phys. Conf. Ser. 1272 012012Document9 pagesGonzález-Correa 2019 J. Phys. Conf. Ser. 1272 012012jeovanniNo ratings yet
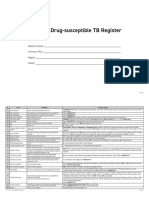
- Form 6a. Drug Susceptible TB RegisterDocument4 pagesForm 6a. Drug Susceptible TB RegisterAllen ChesterNo ratings yet
- Current Challenges With Inflation in NigeriaDocument23 pagesCurrent Challenges With Inflation in Nigeriajamessabraham2No ratings yet
- Digital Transformation of Healthcare at Singapore's Juroaghealth ServiceDocument3 pagesDigital Transformation of Healthcare at Singapore's Juroaghealth ServiceUsama TahirNo ratings yet
- Mining Engineering NV 2014Document108 pagesMining Engineering NV 2014secretspy100% (5)
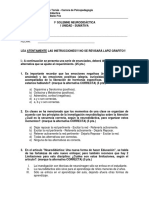
- Universidad Santo Tomás - Carrera de Psicopedagogía - 1a Solemne NeurodidácticaDocument4 pagesUniversidad Santo Tomás - Carrera de Psicopedagogía - 1a Solemne NeurodidácticaPatricio Andrés BelloNo ratings yet
- LABORATORY SAFETY: A Self-Assessment Workbook - CHAPTERS 1 & 2Document5 pagesLABORATORY SAFETY: A Self-Assessment Workbook - CHAPTERS 1 & 2PA2014No ratings yet
- Chapter 2 Social Demography PPT (Autosaved)Document35 pagesChapter 2 Social Demography PPT (Autosaved)Mannat BindraNo ratings yet
- Family Psychology QuestionnaireDocument5 pagesFamily Psychology QuestionnairemuffinshuffleeffieNo ratings yet
- Short Answer Type QuestionsDocument3 pagesShort Answer Type QuestionsDhiman DeyNo ratings yet
- EMT Refresher FlyerDocument2 pagesEMT Refresher FlyerBillR.YoungNo ratings yet
- Endoftalmitis EndogenaDocument1 pageEndoftalmitis EndogenaAlexander Fabián Rodríguez DíazNo ratings yet
- PD0B-501 Details of Test Code For System PackDocument2 pagesPD0B-501 Details of Test Code For System PackVikram SinghNo ratings yet
- International Journal of Biological & Medical Research: Case ReportDocument3 pagesInternational Journal of Biological & Medical Research: Case ReportAndreea Diana DrăgoiNo ratings yet
- Oe23111497121Document3 pagesOe23111497121mohamedNo ratings yet
- Vegan. The Healthiest Diet. Henrich, Ernst WalterDocument42 pagesVegan. The Healthiest Diet. Henrich, Ernst Walteralice1605No ratings yet
- Ti O2Document4 pagesTi O2Muhamad Fahmi Dermawan EndonesyNo ratings yet
- Form 10K-HNTDocument170 pagesForm 10K-HNTNeicy WilsonNo ratings yet
- Every Child Matters PDF 2003Document2 pagesEvery Child Matters PDF 2003AshleyNo ratings yet
- Republic V Cagandahan DigestDocument2 pagesRepublic V Cagandahan DigestJustin Paras100% (1)
- Health Psychology Canadian 4Th Edition Taylor Solutions Manual Full Chapter PDFDocument27 pagesHealth Psychology Canadian 4Th Edition Taylor Solutions Manual Full Chapter PDFalanquangfmrw100% (9)
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- Ganesh Genesis Fire: Case StudyDocument22 pagesGanesh Genesis Fire: Case StudyAshishNo ratings yet
- The Belly Fat Diet John ChathamDocument92 pagesThe Belly Fat Diet John ChathamGurpreet Kaur100% (3)
- Skill Lab Articles As Per Inc Price ListDocument10 pagesSkill Lab Articles As Per Inc Price ListAmanjot SinghNo ratings yet
- Health Education: Quarter 1 - Module 1: Health Information, Products and ServicesDocument29 pagesHealth Education: Quarter 1 - Module 1: Health Information, Products and ServicesNana TempestNo ratings yet
- IMCI Session 2 - An Overview of The IMCIDocument37 pagesIMCI Session 2 - An Overview of The IMCIsarguss14100% (3)
- Rekap Resep - 2021-03-01T160848.881Document2,906 pagesRekap Resep - 2021-03-01T160848.881Dhita AnaleptaNo ratings yet
- Candela Gentle Pro - 16026752105746Document6 pagesCandela Gentle Pro - 16026752105746Andrea Mejia100% (1)
- Manajemen Pada ObesitasDocument11 pagesManajemen Pada ObesitasahmadNo ratings yet
- MSDS MnO2Document6 pagesMSDS MnO2fajarismanadiaNo ratings yet