You might also like
- Cherenkov RadiationDocument17 pagesCherenkov RadiationMayank GargNo ratings yet
- Eurados Report 201202Document194 pagesEurados Report 201202Laurentiu RadoiNo ratings yet
- Handbook of Industrial Mixing-Science and Practice (Book Review)Document3 pagesHandbook of Industrial Mixing-Science and Practice (Book Review)Imane ARNo ratings yet
- Thesis On TWTDocument181 pagesThesis On TWTarshad aliNo ratings yet
- Materials Analysis by Ion Channeling: Submicron CrystallographyFrom EverandMaterials Analysis by Ion Channeling: Submicron CrystallographyNo ratings yet
- The Radiation Chemistry of MacromoleculesFrom EverandThe Radiation Chemistry of MacromoleculesMalcolm DoleNo ratings yet
- 3D Dose Computation AlgorithmsDocument10 pages3D Dose Computation AlgorithmsHashir SaeedNo ratings yet
- 9 Item PDFDocument10 pages9 Item PDFandreaNo ratings yet
- Generalized Integrating Sphere TheoryDocument4 pagesGeneralized Integrating Sphere Theorybumbacumba0% (1)
- Icru 82Document67 pagesIcru 82Aditya DisdusNo ratings yet
- Nuclear Medicine Inc.'s Iodine Value Chain AnalysisDocument6 pagesNuclear Medicine Inc.'s Iodine Value Chain AnalysisPrashant NagpureNo ratings yet
- A Minimalist Flocking Algorithm For Swarm Robots PDFDocument8 pagesA Minimalist Flocking Algorithm For Swarm Robots PDFMayyank GargNo ratings yet
- Body MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveDocument19 pagesBody MRI Artifacts in Clinical Practice: A Physicist's and Radiologist's PerspectiveaegysabetterwayNo ratings yet
- Msa NejmDocument15 pagesMsa NejmSantosh DashNo ratings yet
- Agility MLC Transmission Optimization in The MonacoDocument10 pagesAgility MLC Transmission Optimization in The MonacoLuis Felipe LimasNo ratings yet
- Senior Radiographer Nuclear MedicineDocument1 pageSenior Radiographer Nuclear Medicinetafi66No ratings yet
- Design, Construction and NMR Testing of A 1 Tesla Halbach Permanent Magnet For Magnetic ResonanceDocument5 pagesDesign, Construction and NMR Testing of A 1 Tesla Halbach Permanent Magnet For Magnetic Resonancearesnickety100% (3)
- TG 244 Anal Write UpDocument14 pagesTG 244 Anal Write Upapi-347149977No ratings yet
- ICRU Report 10bDocument115 pagesICRU Report 10bЕвгений ГольдманNo ratings yet
- Basic Considerations in Nuclear MedicineDocument12 pagesBasic Considerations in Nuclear Medicinechberg13No ratings yet
- Mixer Module Users Guide PDFDocument136 pagesMixer Module Users Guide PDFRene D. ArrietaNo ratings yet
- European Guidelines Quality Criteria Computed Tomography Eur 16252Document114 pagesEuropean Guidelines Quality Criteria Computed Tomography Eur 16252Thanh BaronNo ratings yet
- AAPM 34 - MRI Acceptance TestDocument16 pagesAAPM 34 - MRI Acceptance TestmahbodsedNo ratings yet
- Quantec Aamd PDFDocument41 pagesQuantec Aamd PDFNika TopuriaNo ratings yet
- Huq CT SimulatorDocument65 pagesHuq CT SimulatorEskadmas BelayNo ratings yet
- Review of Moving Object Segmentation TechniquesDocument29 pagesReview of Moving Object Segmentation TechniquesMonique PadovanNo ratings yet
- Resolving Major Global Environmental Issues by 2030Document3 pagesResolving Major Global Environmental Issues by 2030Nare BalyanNo ratings yet
- Mutual Coupling in Antenna Arrays: Guest Editors: Hon Tat Hui, Marek E. Bialkowski, and Hoi Shun LuiDocument94 pagesMutual Coupling in Antenna Arrays: Guest Editors: Hon Tat Hui, Marek E. Bialkowski, and Hoi Shun LuiMd AhmedNo ratings yet
- 2005 Magnetom Flash 2 2Document52 pages2005 Magnetom Flash 2 2Herick SavioneNo ratings yet
- Nuclear Medicine GuideDocument3 pagesNuclear Medicine GuidejeffsunilNo ratings yet
- Big Data and Climate Change: Hossein Hassani, Xu Huang and Emmanuel SilvaDocument17 pagesBig Data and Climate Change: Hossein Hassani, Xu Huang and Emmanuel SilvaBL OeiNo ratings yet
- Academic Medical Accelerators Revised2Document50 pagesAcademic Medical Accelerators Revised2sushmita singhNo ratings yet
- Vant Hof SpringerProtocols 2019 V2finalDocument38 pagesVant Hof SpringerProtocols 2019 V2finalSusi SusantiNo ratings yet
- Allreports PDFDocument2 pagesAllreports PDFNeena SinghNo ratings yet
- 1987 - ST John - Aseismic Design of Underground Structures PDFDocument33 pages1987 - ST John - Aseismic Design of Underground Structures PDFpouyaNo ratings yet
- Task Group No. 43-U1Document44 pagesTask Group No. 43-U1fazli.samarNo ratings yet
- NEL FFT Suite User GuideDocument18 pagesNEL FFT Suite User GuideCristian VogelNo ratings yet
- SPATIAL ENCODING WITH GRADIENTS IN MRIDocument26 pagesSPATIAL ENCODING WITH GRADIENTS IN MRIwisesoar100% (1)
- Space Ordnance Systems and Pyrotechnics: An Overview of Key Concepts and ApplicationsDocument91 pagesSpace Ordnance Systems and Pyrotechnics: An Overview of Key Concepts and ApplicationsElumalai SrinivasanNo ratings yet
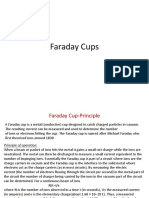
- Faraday CupsDocument10 pagesFaraday CupsAshish SharmaNo ratings yet
- myQA Daily Users GuideDocument87 pagesmyQA Daily Users GuideDaniela ZanchiNo ratings yet
- F-18 NaFDocument47 pagesF-18 NaFLadipo Temitope AyodejiNo ratings yet
- Csi Plan Writeup Portion Turn in PDFDocument13 pagesCsi Plan Writeup Portion Turn in PDFapi-481226212No ratings yet
- Black Box ReportDocument24 pagesBlack Box ReportYashasCRNo ratings yet
- Aapm Report No.166Document70 pagesAapm Report No.166samuelfsjNo ratings yet
- User Manual for 2D-ARRAYXDR and ARRAY INTERFACEXDRDocument27 pagesUser Manual for 2D-ARRAYXDR and ARRAY INTERFACEXDRJorge CifuentesNo ratings yet
- Lung Cancer and Lung Nodules - An IntroductionDocument5 pagesLung Cancer and Lung Nodules - An Introductionpurushothaman sinivasan100% (1)
- Phy ChemDocument248 pagesPhy ChemBitter SugarNo ratings yet
- Csi - Glenda LongoriaDocument11 pagesCsi - Glenda Longoriaapi-302707617No ratings yet
- Treatment Planning Heterogeneity Vs Homogeneity Lung ProjectDocument13 pagesTreatment Planning Heterogeneity Vs Homogeneity Lung Projectapi-299138743No ratings yet
- ICRU 29 Dose Specification For Reporting External Beam Therapy With Photons and Electrons PDFDocument29 pagesICRU 29 Dose Specification For Reporting External Beam Therapy With Photons and Electrons PDFDiego MauricioNo ratings yet
- ICRU Report 62 Prescribing Recording and Reporting Photon Beam Therapy (Supplment To ICRU Report 50)Document62 pagesICRU Report 62 Prescribing Recording and Reporting Photon Beam Therapy (Supplment To ICRU Report 50)Jose Miguel Oyarzun SilvaNo ratings yet
- Thermobaric Effects Formed by Aluminum Foils Enveloping Cylindrical ChargesDocument10 pagesThermobaric Effects Formed by Aluminum Foils Enveloping Cylindrical ChargesAnonymous QFUEsUAnNo ratings yet
- Radiation Health Protection ManualDocument58 pagesRadiation Health Protection Manualgangzhu liangNo ratings yet
- GL Principles and Practice of PET-CT Part 1Document101 pagesGL Principles and Practice of PET-CT Part 1Victoria Lopez RodriguezNo ratings yet
- Vessel VolumesDocument61 pagesVessel VolumesaliNo ratings yet
- 3.1.3.4 Phase I EDD 18-0641.01 Colleferro Rev05 TextDocument50 pages3.1.3.4 Phase I EDD 18-0641.01 Colleferro Rev05 Textfanta calcioNo ratings yet
- Automated Radiation Treatment Planning For CervicaDocument8 pagesAutomated Radiation Treatment Planning For CervicaPutripurwo8664No ratings yet
- Ojsadmin, 202Document6 pagesOjsadmin, 202adejumo2962No ratings yet
- Is Volume Transfer Coefficient (K) Related To Histologic Grade in Human Gliomas?Document11 pagesIs Volume Transfer Coefficient (K) Related To Histologic Grade in Human Gliomas?ricky rdnNo ratings yet
- Bitcoin Template 16x9Document5 pagesBitcoin Template 16x9ricky rdnNo ratings yet
- Acute Ischaemic Stroke PDFDocument8 pagesAcute Ischaemic Stroke PDFricky rdnNo ratings yet
- Acute Ischaemic Stroke PDFDocument8 pagesAcute Ischaemic Stroke PDFricky rdnNo ratings yet
- Perfusion and Vascular Permeability: Basic Concepts and Measurement in Dce-Ct and Dce-MriDocument18 pagesPerfusion and Vascular Permeability: Basic Concepts and Measurement in Dce-Ct and Dce-Mriricky rdnNo ratings yet
- Cisterns of BrainDocument50 pagesCisterns of Brainricky rdnNo ratings yet
- 3 Silhouet SignDocument79 pages3 Silhouet Signricky rdnNo ratings yet
- Panduan Pemeriksaan FisikDocument89 pagesPanduan Pemeriksaan Fisikandika0% (1)
- Imaging Approach Malignant Bone Tumor PDFDocument13 pagesImaging Approach Malignant Bone Tumor PDFricky rdnNo ratings yet
- Head Trauma Chapter 6Document43 pagesHead Trauma Chapter 6Aray Al-AfiqahNo ratings yet
- Review of Cancer Research Article From SciencedirectDocument38 pagesReview of Cancer Research Article From SciencedirectRoxana Cristina PopescuNo ratings yet
- Short Bowel Syndrome PDFDocument62 pagesShort Bowel Syndrome PDFricky rdnNo ratings yet
- Crash RespiratoryDocument245 pagesCrash Respiratoryridin007100% (5)
- Diagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFDocument13 pagesDiagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFricky rdnNo ratings yet
- Basic UltrasoundDocument35 pagesBasic Ultrasoundricky rdnNo ratings yet
- Clin Management Thyroid Nodule Eval Web AlgorithmDocument4 pagesClin Management Thyroid Nodule Eval Web Algorithmricky rdnNo ratings yet
- Why Clinical Radiology As A Career 0Document4 pagesWhy Clinical Radiology As A Career 0ricky rdnNo ratings yet
- 14 15 XII Chem Organic ChaptDocument2 pages14 15 XII Chem Organic ChaptsubiNo ratings yet
- Reflection Paper #1 - Introduction To Action ResearchDocument1 pageReflection Paper #1 - Introduction To Action Researchronan.villagonzaloNo ratings yet
- Individual Sports Prelim ExamDocument13 pagesIndividual Sports Prelim ExamTommy MarcelinoNo ratings yet
- Development of Rsto-01 For Designing The Asphalt Pavements in Usa and Compare With Aashto 1993Document14 pagesDevelopment of Rsto-01 For Designing The Asphalt Pavements in Usa and Compare With Aashto 1993pghasaeiNo ratings yet
- Problems of Teaching English As A Foreign Language in YemenDocument13 pagesProblems of Teaching English As A Foreign Language in YemenSabriThabetNo ratings yet
- Device Interface Device Type (Router, Switch, Host) IP Address Subnet Mask Default GatewayDocument2 pagesDevice Interface Device Type (Router, Switch, Host) IP Address Subnet Mask Default GatewayRohit Chouhan0% (1)
- Biomotor Development For Speed-Power Athletes: Mike Young, PHD Whitecaps FC - Vancouver, BC Athletic Lab - Cary, NCDocument125 pagesBiomotor Development For Speed-Power Athletes: Mike Young, PHD Whitecaps FC - Vancouver, BC Athletic Lab - Cary, NCAlpesh Jadhav100% (1)
- Desert Power India 2050Document231 pagesDesert Power India 2050suraj jhaNo ratings yet
- S2 Retake Practice Exam PDFDocument3 pagesS2 Retake Practice Exam PDFWinnie MeiNo ratings yet
- Inventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Document10 pagesInventarisasi Data Kondisi Jalan Ke Dalam Aplikasi Sistem Informasi Geografis (Sig)Wiro SablengNo ratings yet
- Capacity PlanningDocument19 pagesCapacity PlanningfarjadarshadNo ratings yet
- SQL Server 2008 Failover ClusteringDocument176 pagesSQL Server 2008 Failover ClusteringbiplobusaNo ratings yet
- Wacker Neuson RTDocument120 pagesWacker Neuson RTJANUSZ2017100% (4)
- 2002, Vol.86, Issues 4, Hospital MedicineDocument221 pages2002, Vol.86, Issues 4, Hospital MedicineFaisal H RanaNo ratings yet
- A General Guide To Camera Trapping Large Mammals in Tropical Rainforests With Particula PDFDocument37 pagesA General Guide To Camera Trapping Large Mammals in Tropical Rainforests With Particula PDFDiego JesusNo ratings yet
- Machine Learning: Bilal KhanDocument26 pagesMachine Learning: Bilal KhanBilal KhanNo ratings yet
- Timely characters and creatorsDocument4 pagesTimely characters and creatorsnschober3No ratings yet
- THE PEOPLE OF FARSCAPEDocument29 pagesTHE PEOPLE OF FARSCAPEedemaitreNo ratings yet
- Victron MultiPlus 48 1200-13-16 Datasheet enDocument1 pageVictron MultiPlus 48 1200-13-16 Datasheet enBAHJARI AMINENo ratings yet
- WhatsoldDocument141 pagesWhatsoldLuciana KarajalloNo ratings yet
- Major Bank Performance IndicatorsDocument35 pagesMajor Bank Performance IndicatorsAshish MehraNo ratings yet
- JSA - 0026 Chipping & Granite cutting and lying Work At PB-19Document2 pagesJSA - 0026 Chipping & Granite cutting and lying Work At PB-19Koneti JanardhanaraoNo ratings yet
- Driving Continuous Improvement by Developing and Leveraging Lean Key Performance IndicatorsDocument10 pagesDriving Continuous Improvement by Developing and Leveraging Lean Key Performance IndicatorskellendadNo ratings yet
- Boiler Check ListDocument4 pagesBoiler Check ListFrancis VinoNo ratings yet
- Um 0ah0a 006 EngDocument1 pageUm 0ah0a 006 EngGaudencio LingamenNo ratings yet
- Failure Analysis Case Study PDFDocument2 pagesFailure Analysis Case Study PDFScott50% (2)
- Judge Vest Printable PatternDocument24 pagesJudge Vest Printable PatternMomNo ratings yet
- Urodynamics Griffiths ICS 2014Document198 pagesUrodynamics Griffiths ICS 2014nadalNo ratings yet
- Control SystemsDocument269 pagesControl SystemsAntonis SiderisNo ratings yet
- NPV Irr ArrDocument16 pagesNPV Irr ArrAnjaliNo ratings yet