You might also like
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaNo ratings yet
- Claims Form For New India AssuranceDocument2 pagesClaims Form For New India AssuranceRafael BlackNo ratings yet
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- 10 New India Assurance Company - Reimbursement Claim FormDocument3 pages10 New India Assurance Company - Reimbursement Claim FormbhurajeshNo ratings yet
- Fixed Claim FormDocument2 pagesFixed Claim FormVikas GiriNo ratings yet
- National Insurance Company LimitedDocument4 pagesNational Insurance Company Limitedkaransandesara777No ratings yet
- New India Assurance Hospitalisation Claim FormDocument3 pagesNew India Assurance Hospitalisation Claim Formharshmanu1612No ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- HhhDocument4 pagesHhhMcnet WideNo ratings yet
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- In-Patient Claim FormDocument2 pagesIn-Patient Claim Formfaisal_1241No ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakNo ratings yet
- Adamjee Insurance ClaimDocument2 pagesAdamjee Insurance ClaimubaidNo ratings yet
- Kolkata Claim Form - MD-IndiaDocument4 pagesKolkata Claim Form - MD-Indiadipankar0majumderNo ratings yet
- Medical Claim Form (Reimbursement Only)Document2 pagesMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- Claim form for Niramaaya health insuranceDocument2 pagesClaim form for Niramaaya health insuranceu409023No ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- Bajaj Allianz Cashless Request FormDocument3 pagesBajaj Allianz Cashless Request FormM/s MicrotechNo ratings yet
- Pre Authorization Form IHealthcareDocument2 pagesPre Authorization Form IHealthcarecooljack08100% (1)
- MDINDIA Healthcare Services Claim Form GuideDocument4 pagesMDINDIA Healthcare Services Claim Form GuideShubakar ReddyNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Others Claim FormDocument5 pagesOthers Claim FormArvind RayNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument5 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormrhvenkatNo ratings yet
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- Claim FormDocument5 pagesClaim Formsoumyadeep19478425No ratings yet
- Details of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument5 pagesDetails of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ASumitThoratNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- Claim Form NewDocument4 pagesClaim Form NewVicky GautamNo ratings yet
- f5192 PDFDocument2 pagesf5192 PDFVishal AggawalNo ratings yet
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiNo ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- ChecklistDocument9 pagesChecklistkarthikfuser0183No ratings yet
- Mediclaim FormDocument1 pageMediclaim Formpicrush2pmNo ratings yet
- UIICHdfc ClaimformDocument2 pagesUIICHdfc ClaimformdomyomglolNo ratings yet
- COVID-19 Vaccine Consent FormDocument2 pagesCOVID-19 Vaccine Consent FormApurva PathakNo ratings yet
- Critical Illness Claim FormDocument23 pagesCritical Illness Claim FormHihiNo ratings yet
- Personal Accident Claim FormDocument5 pagesPersonal Accident Claim FormMadhava Reddy MunagalaNo ratings yet
- Memorial Hermann Discharge Papers - 3Document5 pagesMemorial Hermann Discharge Papers - 3Alaska JamesNo ratings yet
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceAhmad Zubair40% (5)
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceJawad MuhammadNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormKeerthi PramodhNo ratings yet
- Medical Reimbursement FormDocument2 pagesMedical Reimbursement FormMEMOONA ASHARNo ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 pagesMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviNo ratings yet
- Attending Physician's Statement for Death ClaimDocument2 pagesAttending Physician's Statement for Death ClaimKen CelesteNo ratings yet
- Heritage Health - Pre Auth FormDocument6 pagesHeritage Health - Pre Auth FormBOOKREADER_NOWNo ratings yet
- Clinical Volunteer ApplicationDocument3 pagesClinical Volunteer ApplicationAnonymous tS0WWCCNo ratings yet
- Patient Information Sheet 091409Document2 pagesPatient Information Sheet 091409api-16816262No ratings yet
- FGH Claim Form - May 2014Document2 pagesFGH Claim Form - May 2014vijayNo ratings yet
- Last First Middle InitialDocument3 pagesLast First Middle InitialAsjsjsjsNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: 4 T' Block, Jayanagar, Bangalore - 560 041Document3 pagesRajiv Gandhi University of Health Sciences, Karnataka: 4 T' Block, Jayanagar, Bangalore - 560 041BUVISANTHANo ratings yet
- Kochi Claim FormDocument4 pagesKochi Claim FormRadhika ShenoiNo ratings yet
- Accidental Injury Claim Claimant's Statement: Form A'Document5 pagesAccidental Injury Claim Claimant's Statement: Form A'krishanthapa01No ratings yet
- UIIC ClaimFormDocument2 pagesUIIC ClaimFormkarthikvel80No ratings yet
- NSTUMP - Proposal FormDocument7 pagesNSTUMP - Proposal FormJagadeesh MaheshNo ratings yet
- MAP Application Form (Rev20230719)Document3 pagesMAP Application Form (Rev20230719)Jen EugenioNo ratings yet
- Civil Boq AiiapDocument170 pagesCivil Boq AiiapMuhammad ArslanNo ratings yet
- Recent Advances in Mobile Robotics - TopalovDocument464 pagesRecent Advances in Mobile Robotics - TopalovBruno MacedoNo ratings yet
- Superelement Modeling-Based Dynamic Analysis of Vehicle Body StructuresDocument7 pagesSuperelement Modeling-Based Dynamic Analysis of Vehicle Body StructuresDavid C HouserNo ratings yet
- Desarmado y Armado de Transmision 950BDocument26 pagesDesarmado y Armado de Transmision 950Bedilberto chableNo ratings yet
- Right To Resist Unlawful ArrestDocument1 pageRight To Resist Unlawful ArrestThoth AtlanteanNo ratings yet
- Getting Started With DAX Formulas in Power BI, Power Pivot, and SSASDocument19 pagesGetting Started With DAX Formulas in Power BI, Power Pivot, and SSASJohn WickNo ratings yet
- Counsel For Plaintiff, Mark Shin: United States District Court Northern District of CaliforniaDocument21 pagesCounsel For Plaintiff, Mark Shin: United States District Court Northern District of CaliforniafleckaleckaNo ratings yet
- Susan Abbotson - Critical Companion To Arthur Miller - A Literary Reference To His Life and Work-Facts On File (2007) PDFDocument529 pagesSusan Abbotson - Critical Companion To Arthur Miller - A Literary Reference To His Life and Work-Facts On File (2007) PDFTaha Tariq0% (1)
- StarletDocument16 pagesStarletMohsen SirajNo ratings yet
- MA5616 V800R311C01 Configuration Guide 02Document741 pagesMA5616 V800R311C01 Configuration Guide 02Mário Sapucaia NetoNo ratings yet
- Examples 5 PDFDocument2 pagesExamples 5 PDFskaderbe1No ratings yet
- The General Agreement On Trade in Services An IntroductionDocument22 pagesThe General Agreement On Trade in Services An IntroductionakyregisterNo ratings yet
- Mercedes B-Class Accessories ListDocument34 pagesMercedes B-Class Accessories ListmuskystoatNo ratings yet
- GFRDDocument9 pagesGFRDLalit NagarNo ratings yet
- Copywirting Secrets From The BibleDocument14 pagesCopywirting Secrets From The BibleRAY EDWARDS100% (2)
- Flex VPNDocument3 pagesFlex VPNAnonymous nFOywQZNo ratings yet
- CEMEX Global Strategy CaseDocument4 pagesCEMEX Global Strategy CaseSaif Ul Islam100% (1)
- ITC Report and Accounts 2016Document276 pagesITC Report and Accounts 2016Rohan SatijaNo ratings yet
- G.R. No. L-54171 October 28, 1980 JEWEL VILLACORTA, Assisted by Her Husband, GUERRERO VILLACORTA, COMPANY, Respondents. TEEHANKEE, Acting C.J.Document6 pagesG.R. No. L-54171 October 28, 1980 JEWEL VILLACORTA, Assisted by Her Husband, GUERRERO VILLACORTA, COMPANY, Respondents. TEEHANKEE, Acting C.J.Lyra Cecille Vertudes AllasNo ratings yet
- Should Always: Exercise 1-1. True or FalseDocument7 pagesShould Always: Exercise 1-1. True or FalseDeanmark RondinaNo ratings yet
- Day / Month / Year: Certificate of No Criminal Conviction Applicant Data Collection Form (LOCAL)Document4 pagesDay / Month / Year: Certificate of No Criminal Conviction Applicant Data Collection Form (LOCAL)Lhea RecenteNo ratings yet
- Lunakleen: Standard Type Hepa FilterDocument1 pageLunakleen: Standard Type Hepa FilterRyan Au YongNo ratings yet
- 02 - AbapDocument139 pages02 - Abapdina cordovaNo ratings yet
- Manual Mue Home RGBDocument8 pagesManual Mue Home RGBJason OrtizNo ratings yet
- HOS Dials in The Driver App - Samsara SupportDocument3 pagesHOS Dials in The Driver App - Samsara SupportMaryNo ratings yet
- Lessee Information StatementDocument1 pageLessee Information Statementmja.carilloNo ratings yet
- A Survey of The Advancing Use and Development of Machine Learning in Smart ManufacturingDocument32 pagesA Survey of The Advancing Use and Development of Machine Learning in Smart Manufacturingbeben_19No ratings yet
- Term Paper Mec 208Document20 pagesTerm Paper Mec 208lksingh1987No ratings yet
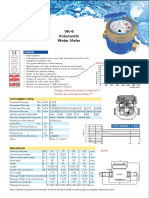
- Baylan: VK-6 Volumetric Water MeterDocument1 pageBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaNo ratings yet
- Moi University: School of Business and EconomicsDocument5 pagesMoi University: School of Business and EconomicsMARION KERUBONo ratings yet
- IFRS 9 and CECL Credit Risk Modelling and Validation: A Practical Guide with Examples Worked in R and SASFrom EverandIFRS 9 and CECL Credit Risk Modelling and Validation: A Practical Guide with Examples Worked in R and SASRating: 3 out of 5 stars3/5 (5)
- University of Berkshire Hathaway: 30 Years of Lessons Learned from Warren Buffett & Charlie Munger at the Annual Shareholders MeetingFrom EverandUniversity of Berkshire Hathaway: 30 Years of Lessons Learned from Warren Buffett & Charlie Munger at the Annual Shareholders MeetingRating: 4.5 out of 5 stars4.5/5 (97)
- Getting Through: Cold Calling Techniques To Get Your Foot In The DoorFrom EverandGetting Through: Cold Calling Techniques To Get Your Foot In The DoorRating: 4.5 out of 5 stars4.5/5 (63)
- Disloyal: A Memoir: The True Story of the Former Personal Attorney to President Donald J. TrumpFrom EverandDisloyal: A Memoir: The True Story of the Former Personal Attorney to President Donald J. TrumpRating: 4 out of 5 stars4/5 (214)
- The Complete Book of Wills, Estates & Trusts (4th Edition): Advice That Can Save You Thousands of Dollars in Legal Fees and TaxesFrom EverandThe Complete Book of Wills, Estates & Trusts (4th Edition): Advice That Can Save You Thousands of Dollars in Legal Fees and TaxesRating: 4 out of 5 stars4/5 (1)
- Buffettology: The Previously Unexplained Techniques That Have Made Warren Buffett American's Most Famous InvestorFrom EverandBuffettology: The Previously Unexplained Techniques That Have Made Warren Buffett American's Most Famous InvestorRating: 4.5 out of 5 stars4.5/5 (132)
- Export & Import - Winning in the Global Marketplace: A Practical Hands-On Guide to Success in International Business, with 100s of Real-World ExamplesFrom EverandExport & Import - Winning in the Global Marketplace: A Practical Hands-On Guide to Success in International Business, with 100s of Real-World ExamplesRating: 5 out of 5 stars5/5 (1)
- Introduction to Negotiable Instruments: As per Indian LawsFrom EverandIntroduction to Negotiable Instruments: As per Indian LawsRating: 5 out of 5 stars5/5 (1)
- The Chickenshit Club: Why the Justice Department Fails to Prosecute ExecutivesWhite Collar CriminalsFrom EverandThe Chickenshit Club: Why the Justice Department Fails to Prosecute ExecutivesWhite Collar CriminalsRating: 5 out of 5 stars5/5 (24)
- Wall Street Money Machine: New and Incredible Strategies for Cash Flow and Wealth EnhancementFrom EverandWall Street Money Machine: New and Incredible Strategies for Cash Flow and Wealth EnhancementRating: 4.5 out of 5 stars4.5/5 (20)
- Dealing With Problem Employees: How to Manage Performance & Personal Issues in the WorkplaceFrom EverandDealing With Problem Employees: How to Manage Performance & Personal Issues in the WorkplaceNo ratings yet
- Ben & Jerry's Double-Dip Capitalism: Lead With Your Values and Make Money TooFrom EverandBen & Jerry's Double-Dip Capitalism: Lead With Your Values and Make Money TooRating: 5 out of 5 stars5/5 (2)
- How to Win a Merchant Dispute or Fraudulent Chargeback CaseFrom EverandHow to Win a Merchant Dispute or Fraudulent Chargeback CaseNo ratings yet
- Richardson's Growth Company Guide 5.0: Investors, Deal Structures, Legal StrategiesFrom EverandRichardson's Growth Company Guide 5.0: Investors, Deal Structures, Legal StrategiesNo ratings yet
- The Chickenshit Club: Why the Justice Department Fails to Prosecute ExecutivesFrom EverandThe Chickenshit Club: Why the Justice Department Fails to Prosecute ExecutivesRating: 5 out of 5 stars5/5 (1)
- Learn the Essentials of Business Law in 15 DaysFrom EverandLearn the Essentials of Business Law in 15 DaysRating: 4 out of 5 stars4/5 (13)
- The Business Legal Lifecycle US Edition: How To Successfully Navigate Your Way From Start Up To SuccessFrom EverandThe Business Legal Lifecycle US Edition: How To Successfully Navigate Your Way From Start Up To SuccessNo ratings yet
- The HR Answer Book: An Indispensable Guide for Managers and Human Resources ProfessionalsFrom EverandThe HR Answer Book: An Indispensable Guide for Managers and Human Resources ProfessionalsRating: 3.5 out of 5 stars3.5/5 (3)