You might also like
- Survival of Children With Sickle Cell DiseaseDocument5 pagesSurvival of Children With Sickle Cell Diseaseapi-3737581100% (1)
- RSCG June03 BriefDocument4 pagesRSCG June03 Briefapi-3737581100% (2)
- Beta Talasemias Nejm PDFDocument12 pagesBeta Talasemias Nejm PDFFiky setiawanNo ratings yet
- Terapia Actual ACFDocument4 pagesTerapia Actual ACFapi-3737581100% (1)
- Screening Newborns For Hemoglobinopathies by HPLCDocument7 pagesScreening Newborns For Hemoglobinopathies by HPLCapi-3737581No ratings yet
- Manejo Del Dolor en ACFDocument3 pagesManejo Del Dolor en ACFapi-3737581No ratings yet
- Sickle Cell Anemia Case Study GuideDocument21 pagesSickle Cell Anemia Case Study GuideLeon0% (1)
- Pnas 0510177103Document5 pagesPnas 0510177103api-3737581No ratings yet
- Supervivencia ACF en ItaliaDocument7 pagesSupervivencia ACF en Italiaapi-3737581No ratings yet
- IAM y HidroxiureaDocument2 pagesIAM y Hidroxiureaapi-3737581No ratings yet
- Post Doctoral Fellowship 2007finalDocument9 pagesPost Doctoral Fellowship 2007finalapi-3737581No ratings yet
- Embedded Secure DocumentDocument1 pageEmbedded Secure Documentapi-3737581No ratings yet
- Disseminated Intravascular CoagulationDocument7 pagesDisseminated Intravascular CoagulationlgebNo ratings yet
- Induccion de HB FetalDocument5 pagesInduccion de HB Fetalapi-3737581No ratings yet
- Hemograma AnormalDocument14 pagesHemograma Anormalapi-3737581No ratings yet
- Disorders of The BloodDocument7 pagesDisorders of The Bloodapi-3737581No ratings yet
- Interleuquina 8Document2 pagesInterleuquina 8api-3737581100% (2)
- Estudio Cooperativo de Anemia Celulas FalciformesDocument12 pagesEstudio Cooperativo de Anemia Celulas Falciformesapi-3737581100% (1)
- Hematopoietic Cell Transplantation ForDocument10 pagesHematopoietic Cell Transplantation Forapi-3737581No ratings yet
- Efecto de La HidroxiuraDocument8 pagesEfecto de La Hidroxiuraapi-3737581No ratings yet
- Deshidratacion en ACFDocument6 pagesDeshidratacion en ACFapi-3737581No ratings yet
- Costing Model For Neonatal Screening and Diagnosis of HaemoglobinopathiesDocument8 pagesCosting Model For Neonatal Screening and Diagnosis of Haemoglobinopathiesapi-3737581No ratings yet
- Beta Talasemias Nejm PDFDocument12 pagesBeta Talasemias Nejm PDFFiky setiawanNo ratings yet
- Correccion de La HBS Por Recombinacion HomologaDocument6 pagesCorreccion de La HBS Por Recombinacion Homologaapi-3737581No ratings yet
- Colelitiasis en Anemia CFDocument6 pagesColelitiasis en Anemia CFapi-3737581No ratings yet
- Banco de SangreDocument1 pageBanco de Sangreapi-3737581No ratings yet
- 2008 Sickle Cell Perf MeasDocument7 pages2008 Sickle Cell Perf Measapi-3737581No ratings yet
- ACF Los IniciosDocument12 pagesACF Los Iniciosapi-3737581No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How To Write AssertionsDocument10 pagesHow To Write AssertionsEden DecierdoNo ratings yet
- Soal Pts 2 Bahasa Inggris XI MIPA & XI IPSDocument3 pagesSoal Pts 2 Bahasa Inggris XI MIPA & XI IPSKhayatul IstiqomahNo ratings yet
- Aspects Between PlanetsDocument35 pagesAspects Between PlanetsbizzoingNo ratings yet
- Stock in Transit (GR - IR Regrouping - Reclassification) - SAP BlogsDocument7 pagesStock in Transit (GR - IR Regrouping - Reclassification) - SAP BlogsusamaNo ratings yet
- Estate court lacks jurisdiction to determine ownership claimsDocument2 pagesEstate court lacks jurisdiction to determine ownership claimsPMV100% (2)
- Active Passive VoiceDocument14 pagesActive Passive VoiceAbhieey Choi Soo HyunNo ratings yet
- (1) 11차 중학영문3800제 3학년 (4쇄) 해설Document64 pages(1) 11차 중학영문3800제 3학년 (4쇄) 해설a01045313124aNo ratings yet
- Bharathidasan University, Tiruchirappalli - 620 024. B.Sc. Zoology - Course Structure Under CBCSDocument21 pagesBharathidasan University, Tiruchirappalli - 620 024. B.Sc. Zoology - Course Structure Under CBCSLeena AneesNo ratings yet
- Pip ProposalDocument4 pagesPip Proposalapi-424238197No ratings yet
- Siemens Sinamics g120 ManualDocument123 pagesSiemens Sinamics g120 ManualWilliam Pereira MartinsNo ratings yet
- Effectiveness of Red Guava Juice in Increasing Erythrocyte Index For Prevention of Anemia in AdolescentsDocument4 pagesEffectiveness of Red Guava Juice in Increasing Erythrocyte Index For Prevention of Anemia in AdolescentsRamayanaNo ratings yet
- Virtualization Software and Linux Installation GuideDocument82 pagesVirtualization Software and Linux Installation GuideshanvijayrNo ratings yet
- Materials Management Functions and EvolutionDocument12 pagesMaterials Management Functions and EvolutionAshok100% (1)
- Full Download Solution Manual For Dynamic Business Law 4th Edition Nancy Kubasek M Neil Browne Linda Barkacs Daniel Herron Carrie Williamson Lucien Dhooge Andrea Giampetro Meyer PDF Full ChapterDocument36 pagesFull Download Solution Manual For Dynamic Business Law 4th Edition Nancy Kubasek M Neil Browne Linda Barkacs Daniel Herron Carrie Williamson Lucien Dhooge Andrea Giampetro Meyer PDF Full Chapterbradleywardxg7pz0100% (17)
- Syllabus TMG 1-0 EASADocument30 pagesSyllabus TMG 1-0 EASAMarc RothNo ratings yet
- Kindred IntroductionDocument18 pagesKindred IntroductionMarionNo ratings yet
- Numerical Analysis of Die Wear Characteristics in Hot Forging of Titanium Alloy Turbine BladeDocument11 pagesNumerical Analysis of Die Wear Characteristics in Hot Forging of Titanium Alloy Turbine BladepinkungNo ratings yet
- A Poetics of Unnatural NarrativeDocument255 pagesA Poetics of Unnatural NarrativeConrad Aquilina100% (5)
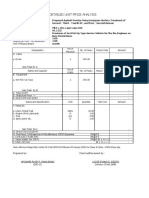
- DETAILED UNIT PRICE ANALYSIS FOR PROPOSED ASPHALT OVERLAYDocument7 pagesDETAILED UNIT PRICE ANALYSIS FOR PROPOSED ASPHALT OVERLAYreynoldNo ratings yet
- Possessive Pronoun FlashcardDocument1 pagePossessive Pronoun FlashcardCelynn ClaireNo ratings yet
- Ang Lampara Ni NenaDocument27 pagesAng Lampara Ni NenaChesee Ann SoperaNo ratings yet
- Assessment of Partially Edentulous Patients BasedDocument9 pagesAssessment of Partially Edentulous Patients BasedEdith Milagros Minaya FloresNo ratings yet
- You Will Increase - Billy Joe DaughertyDocument16 pagesYou Will Increase - Billy Joe DaughertySibil Samuel100% (1)
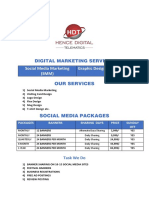
- Digital Marketing Quotation For IndiaDocument3 pagesDigital Marketing Quotation For IndiaBULK SMS PLANSNo ratings yet
- Gradeup's comprehensive guide to teaching and learningDocument6 pagesGradeup's comprehensive guide to teaching and learningRJNo ratings yet
- The Assortment Planning Process GuideDocument7 pagesThe Assortment Planning Process GuidervaraprasadNo ratings yet
- Francis P. DinneenDocument464 pagesFrancis P. DinneenFatima Mirza100% (2)
- Bhimrao Ramji Ambedkar (: (Bimrawramdi Ambe KƏR) ʑ Ɽ ʱ Anthropologist OratorDocument1 pageBhimrao Ramji Ambedkar (: (Bimrawramdi Ambe KƏR) ʑ Ɽ ʱ Anthropologist OratorDevashish ChakrabartyNo ratings yet
- Recreatinal ActivitiesDocument2 pagesRecreatinal ActivitiesRose Ann GrandeNo ratings yet
- National Income MCQsDocument6 pagesNational Income MCQsZeeshan AfzalNo ratings yet