You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ZL 440 Product Data SheetDocument3 pagesZL 440 Product Data SheetVishal ChudasamaNo ratings yet
- Fire Fighting Foam Principles and Ethanol-Blended FuelDocument38 pagesFire Fighting Foam Principles and Ethanol-Blended FuelFrancois HamiauxNo ratings yet
- Electronic Configuration: By: Cyra Eunicer. TanaelDocument17 pagesElectronic Configuration: By: Cyra Eunicer. TanaelDegala, Jan Marlou V.No ratings yet
- Lec 12-Coagulation & FlocculationDocument29 pagesLec 12-Coagulation & FlocculationYaseen YousafNo ratings yet
- The Morse PotentialDocument1 pageThe Morse PotentialPooja SharmaNo ratings yet
- Safety Analysis For The Production of MethanolDocument14 pagesSafety Analysis For The Production of MethanolTauseef Aamere RoseNo ratings yet
- Opc Ecology A3 HL Revision-SheetmodelansDocument1 pageOpc Ecology A3 HL Revision-SheetmodelansFrancisNo ratings yet
- Safety Data Sheet SDS For HIT-RE 500 V3 Epoxy Adhesive Documentation ASSET DOC LOC 5384987Document24 pagesSafety Data Sheet SDS For HIT-RE 500 V3 Epoxy Adhesive Documentation ASSET DOC LOC 5384987Librany RioNo ratings yet
- GENBIO2 - Lesson - The Central Dogma of Molecular BiologyDocument2 pagesGENBIO2 - Lesson - The Central Dogma of Molecular BiologyJazmaine SimbulanNo ratings yet
- Rser D 16 02436R1Document88 pagesRser D 16 02436R1Jitender KaushalNo ratings yet
- Mathematics Arithmetic and Number Sense Algebra Geometry: (Answer Many Word Problems As Possible)Document5 pagesMathematics Arithmetic and Number Sense Algebra Geometry: (Answer Many Word Problems As Possible)DarleneNo ratings yet
- 5982-5753 EUEnglishDocument6 pages5982-5753 EUEnglishcungmapNo ratings yet
- Electrolysis O LevelDocument17 pagesElectrolysis O LevelInnocent EbilNo ratings yet
- Auto 4sem MSEMDocument214 pagesAuto 4sem MSEMkhairnarsayali257No ratings yet
- Properties of LightDocument6 pagesProperties of LightSteffi Bianca U. BelenNo ratings yet
- Selection of Gas CompressorsDocument4 pagesSelection of Gas CompressorsDiegoNo ratings yet
- Green Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlDocument25 pagesGreen Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlteguhwidiartoNo ratings yet
- Science q1 WK 2Document3 pagesScience q1 WK 2Junior FelipzNo ratings yet
- Bolt Torque Calculation For Girth Flange (Ref.: Dennis Moss Procedure 2-10)Document2 pagesBolt Torque Calculation For Girth Flange (Ref.: Dennis Moss Procedure 2-10)Manoj MulikNo ratings yet
- TBP, ASTM, and EFV ComparedDocument2 pagesTBP, ASTM, and EFV Comparedvicktorinox230388No ratings yet
- Crude Analysis - MaxxamDocument2 pagesCrude Analysis - Maxxamgegio60No ratings yet
- Chapter: Semiconductor Electronics: Materials, Devices and Simple Circuits (One Mark Questions)Document19 pagesChapter: Semiconductor Electronics: Materials, Devices and Simple Circuits (One Mark Questions)khannapuneetNo ratings yet
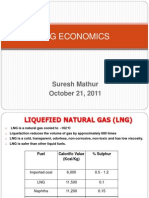
- LNG EconomicsDocument19 pagesLNG EconomicsCal67% (3)
- BL-1400ashless Group 2 03Document2 pagesBL-1400ashless Group 2 03M.ASNo ratings yet
- Practical Chemistry Voumetric EstimationDocument9 pagesPractical Chemistry Voumetric EstimationSanjay Shirodkar100% (2)
- T-Technology Pintér WorksDocument5 pagesT-Technology Pintér Worksmig232323No ratings yet
- Fiitjee: Solutions To JEE (Main) - 2020Document36 pagesFiitjee: Solutions To JEE (Main) - 2020srijan jhaNo ratings yet
- Chem 315 - Lab 5 - Gas Chromatography - AcetatesDocument13 pagesChem 315 - Lab 5 - Gas Chromatography - AcetateskNo ratings yet
- ChapterEight1 - 20 of SpectrocopicDocument20 pagesChapterEight1 - 20 of SpectrocopicHung Le VanNo ratings yet
- Flash Outokumpu Continuous Converting ProcessDocument15 pagesFlash Outokumpu Continuous Converting ProcessSimón BaezaNo ratings yet