You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- DK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFDocument248 pagesDK Publishing - Neal's Yard Remedies Complete Massage - All The Techniques, Disciplines, and Skills You Need To Massage For Wellness (2019, DK) PDFSolveig100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Psychiatry MnemonicsDocument7 pagesPsychiatry MnemonicsFahad Almalki93% (15)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Topographic Anatomy of Basal NucleiDocument44 pagesTopographic Anatomy of Basal NucleiRafique AhmedNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Biomedical InstrumentationDocument16 pagesBiomedical Instrumentationshaswatece100% (6)
- Executive Functions and Frontal Lobe A Conceptual ViewDocument10 pagesExecutive Functions and Frontal Lobe A Conceptual ViewCaroline EchavarriaNo ratings yet
- Dark Room Enlightenment Program OverviewDocument4 pagesDark Room Enlightenment Program OverviewarjunajiNo ratings yet
- Erik Dalton - Myoskeletal Alignment Techniques PDFDocument8 pagesErik Dalton - Myoskeletal Alignment Techniques PDFsuso73100% (2)
- Neuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusDocument17 pagesNeuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusCLAIRE DENISSE DEVISNo ratings yet
- Music TherapyDocument18 pagesMusic TherapyMarylyn Anne AtotNo ratings yet
- Journal TetanusDocument10 pagesJournal TetanusWinariieeyy NayyNo ratings yet
- Neurologic NCLEX Practice Test Part 1Document10 pagesNeurologic NCLEX Practice Test Part 1mpasague100% (2)
- Åyurvedic Check-List: Chaukhambha OrientaliaDocument114 pagesÅyurvedic Check-List: Chaukhambha OrientaliaNirav TrivediNo ratings yet
- Purves Neuroscience Website Questions CH 7 AnswersDocument4 pagesPurves Neuroscience Website Questions CH 7 AnswersPK32145987100% (1)
- Microbiology 2012 13Document101 pagesMicrobiology 2012 13Qurratulain AliNo ratings yet
- The Spinal Cord and Spinal NervesDocument27 pagesThe Spinal Cord and Spinal NervesBelva EdinaNo ratings yet
- History of Neurosurgery in IndonesiaDocument23 pagesHistory of Neurosurgery in IndonesiaPetra O.P. WahjoePramonoNo ratings yet
- By Sweta Kumari Summer Project-II Submitted ToDocument22 pagesBy Sweta Kumari Summer Project-II Submitted ToSudarshanKumar0% (1)
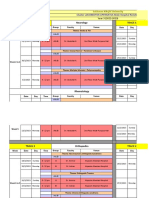
- Sulaiman AlRajhi University Neurology & Orthopedics Hospital Rotation ScheduleDocument10 pagesSulaiman AlRajhi University Neurology & Orthopedics Hospital Rotation ScheduleAbdullah MelhimNo ratings yet
- Neural Control of LocomotionDocument6 pagesNeural Control of LocomotiontanviNo ratings yet
- Arterial Territories of The Human Brain Cerebral HemispheresDocument12 pagesArterial Territories of The Human Brain Cerebral HemispheresErika SanchezNo ratings yet
- 10 Science Notes 07 Control and Coordination 1Document8 pages10 Science Notes 07 Control and Coordination 1All Rounder HindustanNo ratings yet
- Are Fish The Victims of 'Speciesism' A Discussion About Fear, Pain and Animal ConsciousnessDocument12 pagesAre Fish The Victims of 'Speciesism' A Discussion About Fear, Pain and Animal ConsciousnessReuben DylanNo ratings yet
- WBBSE Class IX English SyllabusDocument47 pagesWBBSE Class IX English SyllabusSoumadip MukherjeeNo ratings yet
- The Neurobiology of Thought - The Groundbreaking Discoveries of Patricia Goldman Rakic 1937-2003Document13 pagesThe Neurobiology of Thought - The Groundbreaking Discoveries of Patricia Goldman Rakic 1937-2003juan_bacha_1No ratings yet
- Human Body - Wikipedia PDFDocument18 pagesHuman Body - Wikipedia PDFMavura ZwideNo ratings yet
- CVD Case StudyDocument23 pagesCVD Case StudyMsRhyxelle80% (5)
- Theory of Dreams: All That We See or Seem Is Nothing But A Dream Within A DreamDocument22 pagesTheory of Dreams: All That We See or Seem Is Nothing But A Dream Within A DreamItisikta PaniNo ratings yet
- Surgical Treatment of Traumatic Bifrontal Contusion When and HowDocument37 pagesSurgical Treatment of Traumatic Bifrontal Contusion When and HowNGUYỄN HOÀNG LINHNo ratings yet
- INTRO TO PSYCHOLOGY Assignment No 4 (Depth Perception)Document5 pagesINTRO TO PSYCHOLOGY Assignment No 4 (Depth Perception)Jamal AhmadNo ratings yet
- EEG1Document13 pagesEEG1idno1008No ratings yet