You might also like
- Nasta Pemicu 1 Gawat DaruratDocument21 pagesNasta Pemicu 1 Gawat DaruratThediDarmaWijayaNo ratings yet
- Dafpus Refrat JiwaDocument1 pageDafpus Refrat JiwaThediDarmaWijayaNo ratings yet
- Cover Interna Lapkas 3Document1 pageCover Interna Lapkas 3ThediDarmaWijayaNo ratings yet
- AntihistaminDocument16 pagesAntihistaminThediDarmaWijayaNo ratings yet
- Dr. Surjono W, MSC: Acid - Base BalanceDocument18 pagesDr. Surjono W, MSC: Acid - Base BalanceThediDarmaWijayaNo ratings yet
- Gloria - Kasus 2 Jurnal GenapDocument5 pagesGloria - Kasus 2 Jurnal GenapThediDarmaWijayaNo ratings yet
- Pharmacotherapy of AsthmaDocument40 pagesPharmacotherapy of AsthmaThediDarmaWijayaNo ratings yet
- Thedi - Problem 2ADocument52 pagesThedi - Problem 2AThediDarmaWijayaNo ratings yet
- CKD EvaDocument35 pagesCKD EvaAdhitia MahardikaNo ratings yet
- Kuliah Obat Antiaritmia - ArmenDocument47 pagesKuliah Obat Antiaritmia - ArmenThediDarmaWijayaNo ratings yet
- J 1468-3083 2011 04351 XDocument6 pagesJ 1468-3083 2011 04351 XThediDarmaWijayaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chapter 9 - Managing Crises and National EmergenciesDocument26 pagesChapter 9 - Managing Crises and National EmergenciesJayson TasarraNo ratings yet
- EV3110 SIA Group ReportDocument38 pagesEV3110 SIA Group ReportWill MyatNo ratings yet
- Report On Legal Medicine PowerpointDocument31 pagesReport On Legal Medicine PowerpointEdwin VillaNo ratings yet
- Dapagliflozin Uses, Dosage, Side Effects, WarningsDocument8 pagesDapagliflozin Uses, Dosage, Side Effects, WarningspatgarettNo ratings yet
- Social Welfare Administrartion McqsDocument2 pagesSocial Welfare Administrartion McqsAbd ur Rehman Vlogs & VideosNo ratings yet
- Curriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1Document5 pagesCurriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1joan niniNo ratings yet
- UserGuide2015 PDFDocument114 pagesUserGuide2015 PDFYihan WangNo ratings yet
- Pharmacology Mock Exam MCQDocument8 pagesPharmacology Mock Exam MCQanaeshklNo ratings yet
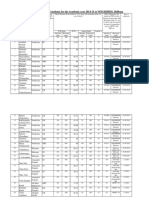
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- Immersion Death: Dr. Rayyan Al-AliDocument42 pagesImmersion Death: Dr. Rayyan Al-AliRayyan AlaliNo ratings yet
- PancreatoblastomaDocument16 pagesPancreatoblastomaDr Farman AliNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiNo ratings yet
- Day Care Center Grant ProposalDocument16 pagesDay Care Center Grant ProposalSaundra100% (1)
- A6013 v1 SD Influenza Ag BrochureDocument2 pagesA6013 v1 SD Influenza Ag BrochureYunescka MorenoNo ratings yet
- Community and Public Health DefinitionsDocument3 pagesCommunity and Public Health DefinitionsSheralyn PelayoNo ratings yet
- 4bi1 - Jan22 2b QPDocument28 pages4bi1 - Jan22 2b QPXIN PEINo ratings yet
- Lasik VisionDocument3 pagesLasik VisionPrachurya SarmaNo ratings yet
- Wellness massage exam questionsDocument3 pagesWellness massage exam questionsElizabeth QuiderNo ratings yet
- Home Economics LiteracyDocument43 pagesHome Economics LiteracyAndrea Fidel Raymundo100% (3)
- 798 3072 1 PBDocument12 pages798 3072 1 PBMariana RitaNo ratings yet
- Interactive CME Teaching MethodsDocument5 pagesInteractive CME Teaching MethodsROMSOPNo ratings yet
- Pit VeriscolorDocument5 pagesPit VeriscolorNida Fithria FadhilaNo ratings yet
- Chirangi vs. StateDocument3 pagesChirangi vs. StateFaithNo ratings yet
- A Case of Eclectic Family TherapyDocument88 pagesA Case of Eclectic Family Therapygun gorNo ratings yet
- Portal Hypertension Clinical Features and ManagementDocument29 pagesPortal Hypertension Clinical Features and ManagementPhilip LingNo ratings yet
- Master Plan for Trivandrum City 2021-2031Document21 pagesMaster Plan for Trivandrum City 2021-2031Adhithy MenonNo ratings yet
- SImOS Nano-Tera 2013Document35 pagesSImOS Nano-Tera 2013nanoteraCHNo ratings yet
- Angle Grinder PDFDocument2 pagesAngle Grinder PDFcityofdarwingisNo ratings yet
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDocument8 pagesAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNo ratings yet
- Transmission Substation Work Practice Manual 2016-07-22Document499 pagesTransmission Substation Work Practice Manual 2016-07-22Edmund YoongNo ratings yet