You might also like
- The Kidney Morphology, Biochemistry, PhysiologyFrom EverandThe Kidney Morphology, Biochemistry, PhysiologyCharles RouillerNo ratings yet
- Bifidobacterium Spp. and Lactobacillus Acidophilus - Biological, Biochemical, Technological and Therapeutical - REVIEW PDFDocument19 pagesBifidobacterium Spp. and Lactobacillus Acidophilus - Biological, Biochemical, Technological and Therapeutical - REVIEW PDFmilu1312No ratings yet
- Immunoregulation in Health and Disease: Experimental and Clinical AspectsFrom EverandImmunoregulation in Health and Disease: Experimental and Clinical AspectsMiodrag L. LukicNo ratings yet
- Newer Methods of Nutritional Biochemistry V5: With Applications and InterpretationsFrom EverandNewer Methods of Nutritional Biochemistry V5: With Applications and InterpretationsAnthony AlbaneseNo ratings yet
- Psychology (Psy10) PowerpointDocument134 pagesPsychology (Psy10) PowerpointEdin AbolenciaNo ratings yet
- 6 Essential NutrientsDocument5 pages6 Essential NutrientsJairo GarciaNo ratings yet
- 3.dietary Surveillance and Nutritional Assessment in England PDFDocument25 pages3.dietary Surveillance and Nutritional Assessment in England PDFAbdul RazakNo ratings yet
- Nature of DiseaseDocument14 pagesNature of DiseaseLambo Ignacio Queen Quin100% (1)
- Biochemical Tests Dietary IntakeDocument10 pagesBiochemical Tests Dietary IntakeDawlat SalamaNo ratings yet
- Nutrition and Functional Foods in Boosting Digestion, Metabolism and Immune HealthFrom EverandNutrition and Functional Foods in Boosting Digestion, Metabolism and Immune HealthNo ratings yet
- Methylenetetrahydrofolate Reductase (MTHFR) Mutation DetectionDocument2 pagesMethylenetetrahydrofolate Reductase (MTHFR) Mutation DetectionRakeshKumarNo ratings yet
- Public Nutrition & Health NCERTDocument15 pagesPublic Nutrition & Health NCERTNidhi SaxenaNo ratings yet
- Biology: Chapter 3-Human Anatomy and PhysiologyDocument7 pagesBiology: Chapter 3-Human Anatomy and PhysiologyMaahrukh Shifa KhanNo ratings yet
- Biometals in Neurodegenerative Diseases: Mechanisms and TherapeuticsFrom EverandBiometals in Neurodegenerative Diseases: Mechanisms and TherapeuticsAnthony R. WhiteRating: 5 out of 5 stars5/5 (1)
- Disorders of Amino Acid MetabolismDocument11 pagesDisorders of Amino Acid MetabolismDiyar AhmadNo ratings yet
- Folic Acid (Vitamin B9), A Simple Guide To The Vitamin, Functions And DeficiencyFrom EverandFolic Acid (Vitamin B9), A Simple Guide To The Vitamin, Functions And DeficiencyRating: 5 out of 5 stars5/5 (1)
- Biochemical MethodDocument35 pagesBiochemical MethodKrizzel Almazora100% (1)
- (Journal of Pediatric Endocrinology and Metabolism) Veganism As A Cause of Iodine Deficient HypothyroidismDocument4 pages(Journal of Pediatric Endocrinology and Metabolism) Veganism As A Cause of Iodine Deficient HypothyroidismFuDanieleNo ratings yet
- Nutrition in Pregnancy Basic Principles and RecommendationsDocument6 pagesNutrition in Pregnancy Basic Principles and RecommendationsAndrea Hinostroza PinedoNo ratings yet
- Inflammation and Immunity in Depression: Basic Science and Clinical ApplicationsFrom EverandInflammation and Immunity in Depression: Basic Science and Clinical ApplicationsBernhard BauneNo ratings yet
- Vegetarian Nutrition 101: The Science Behind a Plant-Based Diet: The Vegetarian Kitchen Series, #3From EverandVegetarian Nutrition 101: The Science Behind a Plant-Based Diet: The Vegetarian Kitchen Series, #3No ratings yet
- What Is NutrigenomicsDocument6 pagesWhat Is NutrigenomicsRitu AilaniNo ratings yet
- Antiphospholipid SyndromeDocument16 pagesAntiphospholipid Syndrometal26No ratings yet
- Amino Acids Interpretive GuideDocument6 pagesAmino Acids Interpretive GuideMetametrix100% (3)
- Ion TransportFrom EverandIon TransportDavid KeelingNo ratings yet
- Inborn Errors of MetabolismDocument27 pagesInborn Errors of MetabolismShelyAzradNo ratings yet
- The Endocrine System LabDocument11 pagesThe Endocrine System Lablaike082921100% (1)
- Intro of Drug-Nutrient InteractionsDocument24 pagesIntro of Drug-Nutrient InteractionsMissBerry25100% (1)
- Nutrition For Patients With Gastrointestinal Disorders Lec 7Document20 pagesNutrition For Patients With Gastrointestinal Disorders Lec 7Youssif MenamNo ratings yet
- Cell of Immunoglobulin SynthesisFrom EverandCell of Immunoglobulin SynthesisBenvenuto PernisNo ratings yet
- Autism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationDocument7 pagesAutism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationSarah Naomi Jeanett ObenhoferNo ratings yet
- Integrative ReviewDocument22 pagesIntegrative Reviewapi-402049640No ratings yet
- Genetic Diseases of the KidneyFrom EverandGenetic Diseases of the KidneyRichard P. LiftonNo ratings yet
- Effects of Urinary CatheterDocument11 pagesEffects of Urinary CatheterAnnis Fathia100% (1)
- Child GERD: Symptoms, Causes and TreatmentsDocument27 pagesChild GERD: Symptoms, Causes and TreatmentsPinkymekala HasanparthyNo ratings yet
- Obesity and Esophageal DisordersFrom EverandObesity and Esophageal DisordersDhyanesh PatelNo ratings yet
- Inborn Error of MetabolismDocument33 pagesInborn Error of MetabolismAlmiraNo ratings yet
- DeVry HIT 111 All Discussions - LatestDocument11 pagesDeVry HIT 111 All Discussions - Latestshonwilllen0% (1)
- Effects of Aging in Endocrine SystemDocument5 pagesEffects of Aging in Endocrine Systemapi-3718174No ratings yet
- Estrogen Metabolism and The Diet-Cancer ConnectionDocument18 pagesEstrogen Metabolism and The Diet-Cancer ConnectionMetametrix100% (1)
- Blood Test and Normal RangeDocument40 pagesBlood Test and Normal Rangeethirukumaran0% (1)
- Case 11-Inflam Bowel - Cronhs D QuestionsDocument9 pagesCase 11-Inflam Bowel - Cronhs D QuestionsAna P.No ratings yet
- Stress and HormonesDocument5 pagesStress and HormonesDiana Espinoza SegoviaNo ratings yet
- Mineral NutritionDocument12 pagesMineral Nutritionsourabh peruriNo ratings yet
- Fact File Gastro Intestinal HormonesDocument2 pagesFact File Gastro Intestinal HormonesSudip DevadasNo ratings yet
- NutraHacker Complete SASDocument9 pagesNutraHacker Complete SASJustin KellyNo ratings yet
- Hair Elements 2013Document5 pagesHair Elements 2013Meghanaram33No ratings yet
- Chinese Medicine For Next Generation HealthcareDocument11 pagesChinese Medicine For Next Generation Healthcarenina_zheng8244No ratings yet
- Analysis of Vegan DietsDocument18 pagesAnalysis of Vegan DietsDemo straviusNo ratings yet
- Introduction To Endocrinology & Endocrine Function Tests.Document14 pagesIntroduction To Endocrinology & Endocrine Function Tests.Junayed Safar MahmudNo ratings yet
- Sialic Acids and Sialoglycoconjugates in the Biology of Life, Health and DiseaseFrom EverandSialic Acids and Sialoglycoconjugates in the Biology of Life, Health and DiseaseNo ratings yet
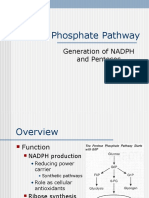
- Pentose Phosphate Pathway: Generation of NADPH and PentosesDocument23 pagesPentose Phosphate Pathway: Generation of NADPH and PentosesV sNo ratings yet
- Diabetes Mellitus Type 2Document3 pagesDiabetes Mellitus Type 2Licio LentimoNo ratings yet
- Endocrinology Learning Goals - IPHY 4440Document9 pagesEndocrinology Learning Goals - IPHY 4440Geline Joy D. SamillanoNo ratings yet
- Eukaryotes: Base of Questions of Krok-1 Exam Medical BiologyDocument54 pagesEukaryotes: Base of Questions of Krok-1 Exam Medical BiologyKarla IngaNo ratings yet
- Classical Homocystinuria Disorder SummaryDocument5 pagesClassical Homocystinuria Disorder Summarymonday125No ratings yet
- Nutrition, Metabolism, and Body Temperature RegulationDocument11 pagesNutrition, Metabolism, and Body Temperature RegulationSNo ratings yet
- Principles of NutritionDocument34 pagesPrinciples of Nutritionfakhribabiker100% (1)
- الحضارة ... العدد الاول من سلسلة عالم المعرفةDocument354 pagesالحضارة ... العدد الاول من سلسلة عالم المعرفةSih AkNo ratings yet
- InsulinDocument100 pagesInsulinfakhribabikerNo ratings yet
- ProposalDocument1 pageProposalfakhribabikerNo ratings yet
- Vitamin DDocument3 pagesVitamin DfakhribabikerNo ratings yet
- Extraction and Purification of Natural Products PDFDocument9 pagesExtraction and Purification of Natural Products PDFharishkumar kakraniNo ratings yet
- Medical GeneticsDocument53 pagesMedical Geneticsfakhribabiker0% (1)
- International SaleDocument13 pagesInternational SalefakhribabikerNo ratings yet
- Livro - Poisoning by Plants, Mycotoxins, and Related ToxinsDocument758 pagesLivro - Poisoning by Plants, Mycotoxins, and Related ToxinsCarol Carvalho Correia100% (3)
- Livro - Poisoning by Plants, Mycotoxins, and Related ToxinsDocument758 pagesLivro - Poisoning by Plants, Mycotoxins, and Related ToxinsCarol Carvalho Correia100% (3)
- Lipids MetabolismDocument11 pagesLipids MetabolismfakhribabikerNo ratings yet
- Assignment No. 5 Peroxisome Proliferator-Activated Receptos PparsDocument1 pageAssignment No. 5 Peroxisome Proliferator-Activated Receptos PparsfakhribabikerNo ratings yet
- English Legal Terminology GlossaryDocument37 pagesEnglish Legal Terminology GlossaryfakhribabikerNo ratings yet
- Extraction and Purification of Natural Products PDFDocument9 pagesExtraction and Purification of Natural Products PDFharishkumar kakraniNo ratings yet
- Functional Groups in Biomolecules PDFDocument5 pagesFunctional Groups in Biomolecules PDFfakhribabikerNo ratings yet
- Contribution To The Flora of Gash Delta, Eastern SudanDocument17 pagesContribution To The Flora of Gash Delta, Eastern SudanfakhribabikerNo ratings yet
- Isomerism in Biomolecules PDFDocument2 pagesIsomerism in Biomolecules PDFfakhribabiker100% (2)
- Sudan IndexDocument614 pagesSudan Indexfakhribabiker100% (3)
- Excel FormulasDocument205 pagesExcel Formulashradmin99100% (33)
- Standard Music Notation PracticeDocument20 pagesStandard Music Notation PracticefakhribabikerNo ratings yet
- (Drug Text) - (PDF) - Drug War FactbookDocument120 pages(Drug Text) - (PDF) - Drug War FactbookMichael LasleyNo ratings yet
- Resaerch MethodologyDocument116 pagesResaerch Methodologyfakhribabiker100% (19)
- Adenosine TriphosphateDocument11 pagesAdenosine TriphosphateAyush LNo ratings yet
- EXPE1Document12 pagesEXPE1K-yanVehraaYomomaNo ratings yet
- JPCL Pipeline Ebook1 PDFDocument27 pagesJPCL Pipeline Ebook1 PDFDorje Phagmo100% (1)
- Active Performance Argan Milk: Drench Skin & Hair in Natural Argan GoodnessDocument2 pagesActive Performance Argan Milk: Drench Skin & Hair in Natural Argan Goodnesscontentdrive4 drive4No ratings yet
- Org ChemDocument172 pagesOrg ChemMikaila Denise LoanzonNo ratings yet
- Restricted Substances List (Apparel, Accessory and Equipment)Document75 pagesRestricted Substances List (Apparel, Accessory and Equipment)abu7omar-1No ratings yet
- Cellular RespirationDocument1 pageCellular RespirationPrecious BalgunaNo ratings yet
- Nexgen Catalogo 2006 FullDocument24 pagesNexgen Catalogo 2006 Fullbresler_linNo ratings yet
- Polyphenol Oxidase Activity and Browning of Three Avocado VarietiesDocument6 pagesPolyphenol Oxidase Activity and Browning of Three Avocado VarietiesMiguelArceMonroyNo ratings yet
- Hirayama HV Series ManualDocument47 pagesHirayama HV Series ManualATR Assistência Técnica (ATR)No ratings yet
- Extraction of Fish Oil From Fish ByproductsA ComparisonDocument11 pagesExtraction of Fish Oil From Fish ByproductsA ComparisonIka Nur FajrianiNo ratings yet
- New Pattr Model Q 01.Document43 pagesNew Pattr Model Q 01.Hari Krishnan KNo ratings yet
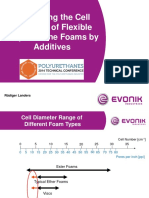
- Influencing The Cell Structure of Flexible Polyurethane Foams by Additives (Presentation) PDFDocument32 pagesInfluencing The Cell Structure of Flexible Polyurethane Foams by Additives (Presentation) PDFСергей ДружининNo ratings yet
- Codex Alimentarius CommissionDocument68 pagesCodex Alimentarius Commissioncurious_leneNo ratings yet
- Balance de MasaDocument18 pagesBalance de MasaMalu BarreraNo ratings yet
- General Organic ChemistryDocument31 pagesGeneral Organic Chemistryshitaldr767No ratings yet
- Complexometric Titrations by Gunja ChaturvediDocument16 pagesComplexometric Titrations by Gunja ChaturvediGunja Chaturvedi100% (3)
- Organic Chemistry Laboratory: Report 6: Reflux ReactionDocument7 pagesOrganic Chemistry Laboratory: Report 6: Reflux ReactionPhú NguyễnNo ratings yet
- Isolation and Characterization of Saponins From Moringa OleiferaDocument10 pagesIsolation and Characterization of Saponins From Moringa OleiferaAhsani ZakyNo ratings yet
- Elena Petricci and Maurizio Taddei - Microwave Assisted Reactions With Gas ReagentsDocument5 pagesElena Petricci and Maurizio Taddei - Microwave Assisted Reactions With Gas ReagentsnnnnjwNo ratings yet
- Lecture Planner Organic Chemistry PDF Only 12th Board Booster 2024Document2 pagesLecture Planner Organic Chemistry PDF Only 12th Board Booster 2024Prince YadavNo ratings yet
- Newman Projections Practice Problems-AnswersDocument4 pagesNewman Projections Practice Problems-AnswersNatasha Nadya Hussin100% (1)
- Section 08500 - Windows: Whole Building Design Guide Federal Green Construction Guide For SpecifiersDocument7 pagesSection 08500 - Windows: Whole Building Design Guide Federal Green Construction Guide For SpecifiersAnonymous NMytbMiDNo ratings yet
- Obat Paten Slow Moving 2-DikonversiDocument1 pageObat Paten Slow Moving 2-Dikonversininil widiyastutikNo ratings yet
- Aromatic Electrophilic SubstitutionDocument71 pagesAromatic Electrophilic SubstitutionsridharancNo ratings yet
- Sicilian Lemon OilDocument12 pagesSicilian Lemon OilbabithyNo ratings yet
- Reagen Lab Reorder ListDocument3 pagesReagen Lab Reorder ListlabNo ratings yet
- A Systematic Review of The Life Cycle Environmental Performance of CottonDocument10 pagesA Systematic Review of The Life Cycle Environmental Performance of Cottonivory11136999No ratings yet
- OBdTC Sdit. Preliminary and Confirmatory TestsDocument7 pagesOBdTC Sdit. Preliminary and Confirmatory TestsSrushti ChouguleNo ratings yet
- Chapter 14 Weathering and ErosionDocument34 pagesChapter 14 Weathering and ErosionValentina LópezNo ratings yet