You might also like
- Viral Exanthems: Sahara Tuazan AbonawasDocument75 pagesViral Exanthems: Sahara Tuazan AbonawasMarlon Cenabre Turaja100% (1)
- Measles: A Highly Contagious Viral DiseaseDocument2 pagesMeasles: A Highly Contagious Viral DiseaseKAREEM WAHEEDNo ratings yet
- Fever With Rash SeminarDocument98 pagesFever With Rash SeminarSYAZRIANA SUHAIMINo ratings yet
- Classic Childhood ExanthemsDocument66 pagesClassic Childhood ExanthemsBorzoo Tajdin100% (1)
- Meningitis In Children: Signs, Symptoms And TreatmentDocument48 pagesMeningitis In Children: Signs, Symptoms And TreatmentAli FalihNo ratings yet
- Understanding Chlamydiae InfectionsDocument32 pagesUnderstanding Chlamydiae InfectionsNaing Lin SoeNo ratings yet
- Arboviruses: R.Varidianto Yudo T., Dr.,MkesDocument19 pagesArboviruses: R.Varidianto Yudo T., Dr.,MkesalbertmogNo ratings yet
- Tropical Infection DiseasesDocument60 pagesTropical Infection DiseasesVerarisna100% (1)
- Infectious Diseases of The HeartDocument84 pagesInfectious Diseases of The HeartHarold DiasanaNo ratings yet
- Bacterial Skin Infections GuideDocument37 pagesBacterial Skin Infections GuideAngelie PedregosaNo ratings yet
- Infections in Pregnancy FinalDocument67 pagesInfections in Pregnancy FinalkashafNo ratings yet
- NeisseriaDocument32 pagesNeisseriaKeshant SamarooNo ratings yet
- Neurological Manifestations of HIV/AIDSDocument34 pagesNeurological Manifestations of HIV/AIDSashuNo ratings yet
- Gilut Herpes ZosteRDocument24 pagesGilut Herpes ZosteRdimasahadiantoNo ratings yet
- PyomeningitisDocument54 pagesPyomeningitisRiya BagdiNo ratings yet
- Infections in Pregnancy 2Document26 pagesInfections in Pregnancy 2Karanand Choppingboardd Rahgav MaharajNo ratings yet
- 24.11.09 PPT On Intrauterine InfectionDocument57 pages24.11.09 PPT On Intrauterine InfectionDhara Meena90% (10)
- Erythema NodosumDocument42 pagesErythema Nodosummedpedshospitalist100% (1)
- Viral ExanthemsDocument133 pagesViral ExanthemsDesiree AfagaNo ratings yet
- Guide to Dermatomycoses: Fungal Infections of the Skin, Hair and NailsDocument73 pagesGuide to Dermatomycoses: Fungal Infections of the Skin, Hair and NailssnylstlNo ratings yet
- Miliaria SVDocument26 pagesMiliaria SVTaufiq Ramadhan100% (1)
- Chikungunya WDocument11 pagesChikungunya Wapi-378136896100% (1)
- Haemophilus ducreyi causes chancroidDocument15 pagesHaemophilus ducreyi causes chancroidchristieNo ratings yet
- Bacterial Skin Infections GuideDocument41 pagesBacterial Skin Infections GuideUmmi Rinandari100% (1)
- Lecture-4 Viral GastroenteritisDocument37 pagesLecture-4 Viral GastroenteritislolitlolatNo ratings yet
- Skin Manifestations of HIV DiseaseDocument31 pagesSkin Manifestations of HIV Diseaselovelots1234No ratings yet
- Brucellosis 2Document70 pagesBrucellosis 2Zara IftikharNo ratings yet
- Atopic Eczema 11Document71 pagesAtopic Eczema 11khola aijazNo ratings yet
- Leprosy LecDocument26 pagesLeprosy LecAL Babaran CanceranNo ratings yet
- Actinomyces & Nocardia 06-07-MedDocument11 pagesActinomyces & Nocardia 06-07-Medapi-3699361No ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- 11 Spirochetes 130520112830 Phpapp02Document61 pages11 Spirochetes 130520112830 Phpapp02Manisanthosh KumarNo ratings yet
- Chickenpox Info Sheet 20151221Document4 pagesChickenpox Info Sheet 20151221Angelo Trester GuimarasNo ratings yet
- SyphilisDocument89 pagesSyphilisAnuZ13thNo ratings yet
- Approach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCDocument65 pagesApproach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCCristinaConcepcionNo ratings yet
- Dr. Sadeli Masria, DR., SPMK., Ms. DMMDocument64 pagesDr. Sadeli Masria, DR., SPMK., Ms. DMMPraluki HerliawanNo ratings yet
- Differential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesDocument2 pagesDifferential Diagnosis of Rash Illness: Disease Sign/Symptoms Type of Rash Other FeaturesCarlo CondeNo ratings yet
- Opportunistic Amoeba Facultative ParasitesDocument25 pagesOpportunistic Amoeba Facultative ParasitesLizeth Querubin100% (10)
- Vesiculobullous DiseasesDocument40 pagesVesiculobullous Diseasessgoeldoc_550661200100% (1)
- Bacterial MeningitisDocument1 pageBacterial MeningitisDavid HylandNo ratings yet
- Viral InfectionsDocument103 pagesViral InfectionsAkash Anilkumar MaliniNo ratings yet
- Rabies FinalDocument18 pagesRabies FinalPrem SinghNo ratings yet
- Dermatitis and EczemaDocument67 pagesDermatitis and EczemaIts AnythingNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- Erythema MultiformeDocument29 pagesErythema MultiformeSurabhi Sharma100% (1)
- PAPOVIRUSESDocument35 pagesPAPOVIRUSESFrancis MakanyaNo ratings yet
- CNS Infections: Meningitis vs EncephalitisDocument32 pagesCNS Infections: Meningitis vs EncephalitisAzizul Halid100% (1)
- H.influenzae Modified 2012Document12 pagesH.influenzae Modified 2012MoonAIRNo ratings yet
- MILIARIADocument6 pagesMILIARIARien Anggraini RazakNo ratings yet
- Congenital Viral InfectionsDocument43 pagesCongenital Viral Infectionsannie1970100% (1)
- Skin Tumor 1Document30 pagesSkin Tumor 1Vicky Ilda Viantini100% (1)
- TOXOPLASMADocument14 pagesTOXOPLASMAShanu KumariNo ratings yet
- Chicken Pox (Varicella) 2Document18 pagesChicken Pox (Varicella) 2Cherrie AngcaoNo ratings yet
- Virology NotesDocument81 pagesVirology NotesraulNo ratings yet
- Swine Flu Pandemic GuideDocument57 pagesSwine Flu Pandemic GuidemlbonthelineNo ratings yet
- Infectious DermatologyDocument206 pagesInfectious DermatologyAaron Christian Earl VillosoNo ratings yet
- Varicella (Chickenpox) Disease: Chananart Yuakyen: IcnDocument28 pagesVaricella (Chickenpox) Disease: Chananart Yuakyen: IcnKana FajarNo ratings yet
- Lerelyn Case Reading4Document53 pagesLerelyn Case Reading4Ma Lerelyn DatinguinooNo ratings yet
- Fwd. Epi 8Document40 pagesFwd. Epi 8Sumayya ChughtaiNo ratings yet
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDocument52 pagesCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaNo ratings yet
- Communicable Diseases ReviewerDocument13 pagesCommunicable Diseases ReviewerPearl DiBerardinoNo ratings yet
- Philippine Inter-Country Adoption Undertaking and ApplicationDocument4 pagesPhilippine Inter-Country Adoption Undertaking and ApplicationPearl DiBerardinoNo ratings yet
- Guide in Taking NCLEXDocument12 pagesGuide in Taking NCLEXPearl DiBerardinoNo ratings yet
- Pathophysiology of ALL (Diagram)Document3 pagesPathophysiology of ALL (Diagram)Joann100% (77)
- Salwa Maghrabi Teacher Assistant Nursing Department: Prepared byDocument30 pagesSalwa Maghrabi Teacher Assistant Nursing Department: Prepared byPearl DiBerardino100% (1)
- AUSTRALIA Nursing and Midwifery Board Template Instructions To Accreditation AuthoritiesDocument2 pagesAUSTRALIA Nursing and Midwifery Board Template Instructions To Accreditation AuthoritiesPearl DiBerardinoNo ratings yet
- Filipino Style of ManagingDocument1 pageFilipino Style of ManagingPearl DiBerardinoNo ratings yet
- How To Design A QuestionnaireDocument3 pagesHow To Design A QuestionnaireMithun SahaNo ratings yet
- Bradbury Jones StudyDocument18 pagesBradbury Jones StudyPearl DiBerardinoNo ratings yet
- Class Size and Student Outcomes - M. ChingosDocument50 pagesClass Size and Student Outcomes - M. ChingosPearl DiBerardinoNo ratings yet
- Men in NursingDocument6 pagesMen in NursingPearl DiBerardinoNo ratings yet
- Attitudes Towards Male Nurses Study 1983Document141 pagesAttitudes Towards Male Nurses Study 1983Pearl DiBerardinoNo ratings yet
- GENDER and CAREER in NursingDocument9 pagesGENDER and CAREER in NursingPearl DiBerardinoNo ratings yet
- Benner's 5 Stages of Nursing CompetenceDocument1 pageBenner's 5 Stages of Nursing CompetenceMagilas S. SalvacionNo ratings yet
- Atrial Septal DefectDocument2 pagesAtrial Septal DefectPearl DiBerardinoNo ratings yet
- Brain AneurysmDocument8 pagesBrain Aneurysmzairajoy07100% (1)
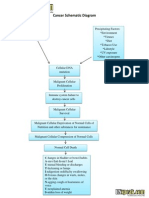
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramPearl DiBerardinoNo ratings yet
- KSA Survey GuideDocument4 pagesKSA Survey GuidePearl DiBerardinoNo ratings yet
- Emotional and Physiologic Elements of Death and DyingDocument17 pagesEmotional and Physiologic Elements of Death and DyinghengkihanggaraNo ratings yet
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramPearl DiBerardinoNo ratings yet
- Lumbar & Sacral VertebraeDocument1 pageLumbar & Sacral VertebraemydewyboyNo ratings yet
- Chapter 12 Health Care of The Older AdultDocument30 pagesChapter 12 Health Care of The Older AdultPearl DiBerardinoNo ratings yet
- Critical CareDocument37 pagesCritical CarePearl DiBerardinoNo ratings yet
- American Cancer Society 2013 TrendsDocument44 pagesAmerican Cancer Society 2013 TrendsPearl DiBerardinoNo ratings yet
- Airway SuctioningDocument30 pagesAirway SuctioningPearl DiBerardinoNo ratings yet
- Tracheostomy Suctioning Procedure GuideDocument1 pageTracheostomy Suctioning Procedure GuidePearl DiBerardinoNo ratings yet
- Evaluation Checklist For Nursing AideDocument2 pagesEvaluation Checklist For Nursing AidePearl DiBerardinoNo ratings yet
- Chapter 17 End-Of-Life CareDocument29 pagesChapter 17 End-Of-Life CarePearl DiBerardinoNo ratings yet
- Chapter 11 Principles and Practices in RehabilitationDocument32 pagesChapter 11 Principles and Practices in RehabilitationPearl DiBerardino100% (1)
- Elevated BilirubinDocument5 pagesElevated BilirubinNovita ApramadhaNo ratings yet
- Vancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsDocument1 pageVancouver Coastal Health Enhanced Surveillance and Precautions ProtocolsIan YoungNo ratings yet
- The China Study PDFDocument7 pagesThe China Study PDFPatrice108365No ratings yet
- Week 29 - DRRRDocument5 pagesWeek 29 - DRRRMira VeranoNo ratings yet
- Evaluation of Fetal HeartDocument59 pagesEvaluation of Fetal Heartاد ريما البدر100% (3)
- Expression of MDM2 and p16 in AngiomyolipomaDocument7 pagesExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresNo ratings yet
- 2.3. Mental Health Nursing: Course DescriptionDocument5 pages2.3. Mental Health Nursing: Course Descriptioncharanjit kaurNo ratings yet
- Lesson 1Document20 pagesLesson 1Irish Jean AgsawayNo ratings yet
- IV Drug ReactionsDocument19 pagesIV Drug Reactionsphp_czarina04421No ratings yet
- Source Control in Emergency General SurgeryDocument21 pagesSource Control in Emergency General SurgerylaviniaNo ratings yet
- OSCE Chart Cough (KK)Document4 pagesOSCE Chart Cough (KK)api-26938624No ratings yet
- Windkessel EffectDocument11 pagesWindkessel EffectAkhmad HidayatNo ratings yet
- Triage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDDocument6 pagesTriage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDRatna SariNo ratings yet
- Erectile DysfunctionDocument145 pagesErectile Dysfunctionluna palitoNo ratings yet
- Assessment and Management of Patients With Hearing and Balance DisordersDocument9 pagesAssessment and Management of Patients With Hearing and Balance Disordersxhemhae100% (1)
- Alzheimer's DiseaseDocument469 pagesAlzheimer's DiseaseGastón G. Fernández100% (3)
- Effects of Malnutrition Among ChildrenDocument3 pagesEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraNo ratings yet
- The Use of Superficial Heat For Treatment of TempoDocument6 pagesThe Use of Superficial Heat For Treatment of TempoJulianaNo ratings yet
- Study On The Efficacy of Nosocomial Infection Control (Senic Project) - Summary of Study DesignDocument14 pagesStudy On The Efficacy of Nosocomial Infection Control (Senic Project) - Summary of Study DesignMunawir GazaliNo ratings yet
- Elevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A NephropathyDocument5 pagesElevated Serum Immunoglobulin E Level As A Marker For Progression Ofimmunoglobulin A Nephropathyagustinaw1981No ratings yet
- Lesson 3 ReviewDocument4 pagesLesson 3 ReviewHo Yong WaiNo ratings yet
- Theory and Practice of Pure Tone Audiometry - PTADocument12 pagesTheory and Practice of Pure Tone Audiometry - PTAsolhazNo ratings yet
- HCCC ComplaintDocument23 pagesHCCC ComplaintPaul GallagherNo ratings yet
- Understanding Traumatic Brain Injury (TBIDocument16 pagesUnderstanding Traumatic Brain Injury (TBIdcNo ratings yet
- DRUG STUDY PsycheDocument1 pageDRUG STUDY Psychejulesubayubay5428100% (1)
- Delafloxacin 4Document23 pagesDelafloxacin 4Muhammad RamzanNo ratings yet
- Health and IllnessDocument2 pagesHealth and IllnessLize Decotelli HubnerNo ratings yet
- Dental Public HealthDocument264 pagesDental Public HealthCorina Manole DanielaNo ratings yet
- Blood and Tissue Coccidian GuideDocument40 pagesBlood and Tissue Coccidian GuideMichael DawitNo ratings yet
- Prevalence of Hypothyroidism in Adults An EpidemioDocument6 pagesPrevalence of Hypothyroidism in Adults An EpidemioCindy Auliah NasutionNo ratings yet