You might also like
- Sedative-Hypnotic DrugsDocument30 pagesSedative-Hypnotic DrugsdrfatimarizNo ratings yet
- 2016 Pharmacology of Sedative-HypnoticDocument46 pages2016 Pharmacology of Sedative-HypnoticFansisca SiallaganNo ratings yet
- Sedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiDocument30 pagesSedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiKAVITA HOODANo ratings yet
- Psychopharmacology: Effects of Drugs on Affect, Cognition and BehaviorDocument101 pagesPsychopharmacology: Effects of Drugs on Affect, Cognition and BehaviorHardeep KaurNo ratings yet
- Sedative - HypnoticsDocument60 pagesSedative - HypnoticsNurul AinNo ratings yet
- CNS Depressants: Sedatives, Hypnotics, and Narcotic AnalgesicsDocument118 pagesCNS Depressants: Sedatives, Hypnotics, and Narcotic Analgesicsbiruk getahunNo ratings yet
- Psychotropic DrugsDocument81 pagesPsychotropic DrugsJoan100% (2)
- Pharmacology of Sedative-HypnoticsDocument49 pagesPharmacology of Sedative-HypnoticsGeorge AbrahamNo ratings yet
- WEEK 6 7-CNS Medications StudentDocument83 pagesWEEK 6 7-CNS Medications Studentx8jdbj5gphNo ratings yet
- Sedative - HypnoticsDocument62 pagesSedative - HypnoticsvijayNo ratings yet
- Sedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityDocument51 pagesSedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityRose Ann Raquiza-PeranteNo ratings yet
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- Sedative Hypnotic PoisoningDocument37 pagesSedative Hypnotic PoisoningDeepa WilliamNo ratings yet
- Introduction To Cns PharmacologyDocument66 pagesIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- نسخة ANTI-ARRHYTHMIC 2Document28 pagesنسخة ANTI-ARRHYTHMIC 2ManWol JangNo ratings yet
- SedativeDocument35 pagesSedativeking_goldNo ratings yet
- Drugs Used in Mental IllnessDocument60 pagesDrugs Used in Mental IllnessDixa MeNo ratings yet
- Antianxiety SedativeDocument44 pagesAntianxiety Sedativemohsen mirdamadiNo ratings yet
- Lecture 28 - 3rd Asessment - Sedatives, HypnoticsDocument32 pagesLecture 28 - 3rd Asessment - Sedatives, Hypnoticsapi-3703352100% (1)
- B2B Psychopharmacology 2015Document128 pagesB2B Psychopharmacology 2015Soleil DaddouNo ratings yet
- Obat-Obat Psychiatry - 1 2018Document104 pagesObat-Obat Psychiatry - 1 2018Christo LimbongNo ratings yet
- Farmacologia Das Drogas Ansiolà TicasDocument65 pagesFarmacologia Das Drogas Ansiolà TicasEduarda StumpfNo ratings yet
- Katzung SummaryDocument60 pagesKatzung Summaryedwarbc1No ratings yet
- Study Guide PNS and CNSDocument7 pagesStudy Guide PNS and CNSsquicciariniNo ratings yet
- Sedative-Hypnotic Drugs: Dr. Hiwa K. Saaed, HD, Msc. PHDDocument51 pagesSedative-Hypnotic Drugs: Dr. Hiwa K. Saaed, HD, Msc. PHDHiwa Khidhir saaedNo ratings yet
- Drug List PsychopharmDocument23 pagesDrug List PsychopharmGeorge HananiaNo ratings yet
- Sedative Hypnotics Anxiolytics Benzodiazepines BarbituratesDocument60 pagesSedative Hypnotics Anxiolytics Benzodiazepines Barbituratesneleh grayNo ratings yet
- Antidepressant DrugsDocument55 pagesAntidepressant Drugsmaheen aurangzaib100% (2)
- Anxiolytics Sedatives Hypnotics Pharm 3Document38 pagesAnxiolytics Sedatives Hypnotics Pharm 3Peter Harris100% (1)
- Second Gen AtipsychoticDocument34 pagesSecond Gen Atipsychoticemamma hashirNo ratings yet
- Psychopharmacological AgentsDocument44 pagesPsychopharmacological Agentsbazet49No ratings yet
- Sedative-Hypnotic Drugs: Mechanisms, Uses, and ToxicityDocument43 pagesSedative-Hypnotic Drugs: Mechanisms, Uses, and Toxicitydave_1128No ratings yet
- AntidepressantsDocument28 pagesAntidepressantsakoeljames8543No ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- AntipsychoticsDocument47 pagesAntipsychoticsammar_ahmed_19No ratings yet
- Psychotherapeutic Drugs GuideDocument12 pagesPsychotherapeutic Drugs Guidecamile buhanginNo ratings yet
- Antidepressants (Igor Iezhitsa) Students Copy (ME219)Document40 pagesAntidepressants (Igor Iezhitsa) Students Copy (ME219)Zobayer AhmedNo ratings yet
- Drug PresentationDocument32 pagesDrug PresentationManisha ShakyaNo ratings yet
- Sedatives and Hypnotics-2Document10 pagesSedatives and Hypnotics-2FRANCA JAMGBADINo ratings yet
- Substance Abuse and Toxins - 20120531Document23 pagesSubstance Abuse and Toxins - 20120531Cindy Van WykNo ratings yet
- Antipsychotic AgentsDocument51 pagesAntipsychotic Agentsakoeljames8543No ratings yet
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 pagesCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92No ratings yet
- Antidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyDocument38 pagesAntidepressant Drugs: Presented By-K.Vinod Dept. of PharmacologyVinod GuruNo ratings yet
- F22 Sedative Hypnotic DrugsDocument37 pagesF22 Sedative Hypnotic DrugsJoyce SumagaysayNo ratings yet
- Antipsychotic DrugsDocument34 pagesAntipsychotic DrugsvimalaNo ratings yet
- Sedative HypnoticsDocument33 pagesSedative HypnoticsIkram HamacheNo ratings yet
- Pharmacology of AntidepressantsDocument28 pagesPharmacology of Antidepressantsحيدر كريم سعيد حمزهNo ratings yet
- Sedative-Hypnotic Drugs GuideDocument21 pagesSedative-Hypnotic Drugs GuideAde ApenkNo ratings yet
- 7 - Anxiolytics-Sedatives-HypnoticsDocument46 pages7 - Anxiolytics-Sedatives-HypnoticsHadeelNo ratings yet
- Depression Medications ExplainedDocument5 pagesDepression Medications ExplainedxyzNo ratings yet
- ANTIDEPRESSANTS MaterialDocument5 pagesANTIDEPRESSANTS MaterialxyzNo ratings yet
- An AntipsychoticDocument4 pagesAn AntipsychoticJoMa TuazonNo ratings yet
- Antiepileptic Drugs ExplainedDocument78 pagesAntiepileptic Drugs ExplainedPrincess VanquirayNo ratings yet
- Topic 2 - TREATMENT OF MENTAL DISEASESDocument52 pagesTopic 2 - TREATMENT OF MENTAL DISEASESprashant singhNo ratings yet
- Antidepressants (ME216) 20 5Document40 pagesAntidepressants (ME216) 20 5Dineish MurugaiahNo ratings yet
- Antipsychotic Drugs - Wafa Bin ShamlanDocument8 pagesAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoNo ratings yet
- The Maudsley Prescribing Guidelines in PsychiatryFrom EverandThe Maudsley Prescribing Guidelines in PsychiatryRating: 5 out of 5 stars5/5 (1)
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionNo ratings yet
- New Text DocumentDocument1 pageNew Text DocumentPande Indra PremanaNo ratings yet
- Study Report DHF and Dengue Fever, Untuk MuatDocument13 pagesStudy Report DHF and Dengue Fever, Untuk MuatPande Indra PremanaNo ratings yet
- Diagnosis Dan Tatalaksana: Nyoman PurwadiDocument26 pagesDiagnosis Dan Tatalaksana: Nyoman PurwadiPande Indra PremanaNo ratings yet
- 8 Rinitis Alergi Eng VersionDocument24 pages8 Rinitis Alergi Eng VersionPande Indra PremanaNo ratings yet
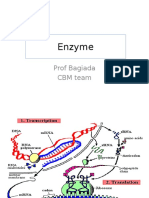
- Enzyme: Prof Bagiada CBM TeamDocument30 pagesEnzyme: Prof Bagiada CBM TeamPande Indra PremanaNo ratings yet
- Alimentary Disorders: Symptoms, Tests, and DiagnosesDocument1 pageAlimentary Disorders: Symptoms, Tests, and DiagnosesPande Indra PremanaNo ratings yet
- Learning Task Alimentary: Self AssessmentDocument1 pageLearning Task Alimentary: Self AssessmentPande Indra PremanaNo ratings yet
- Diagnosis and Management of AmebiasisDocument9 pagesDiagnosis and Management of AmebiasisPande Indra PremanaNo ratings yet
- Upper Alimentary Histology-2012Document23 pagesUpper Alimentary Histology-2012Pande Indra PremanaNo ratings yet
- Upper Alimentary Histology-2012Document23 pagesUpper Alimentary Histology-2012Pande Indra PremanaNo ratings yet
- Toxoplasmosis in PregnancyDocument13 pagesToxoplasmosis in PregnancyPande Indra PremanaNo ratings yet
- 6 ImunoTechniques 2012Document32 pages6 ImunoTechniques 2012Pande Indra PremanaNo ratings yet
- 17 Adrenal GlandDocument33 pages17 Adrenal GlandPande Indra PremanaNo ratings yet
- AA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarDocument26 pagesAA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarPande Indra PremanaNo ratings yet
- 2 Organel LinaDocument34 pages2 Organel LinaMade WidianantaraNo ratings yet
- Doraemon Cartoon Summary: Nobita's Cat Robot Friend From The FutureDocument3 pagesDoraemon Cartoon Summary: Nobita's Cat Robot Friend From The FuturePande Indra PremanaNo ratings yet
- General Principles Physical Exam GuideDocument43 pagesGeneral Principles Physical Exam GuidePande Indra PremanaNo ratings yet
- Uroflowmetry ProcedureDocument1 pageUroflowmetry ProcedurePande Indra PremanaNo ratings yet
- Pathogenesis of Bacterial Infection Sem 3Document46 pagesPathogenesis of Bacterial Infection Sem 3Sheryl ElitaNo ratings yet
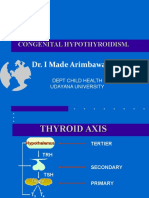
- 19 Congenital HipotiroidDocument21 pages19 Congenital HipotiroidPande Indra PremanaNo ratings yet
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocument38 pagesMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNo ratings yet
- 9 The Balinese TradmedCAMDocument43 pages9 The Balinese TradmedCAMPande Indra PremanaNo ratings yet
- 2 Total Ergonomic ApproachDocument25 pages2 Total Ergonomic ApproachPande Indra PremanaNo ratings yet
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocument38 pagesMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNo ratings yet
- Describe of Definition of PolypharmacyDocument1 pageDescribe of Definition of PolypharmacyPande Indra PremanaNo ratings yet
- 19 Congenital HipotiroidDocument21 pages19 Congenital HipotiroidPande Indra PremanaNo ratings yet
- Treatment of Viral InfectionDocument33 pagesTreatment of Viral InfectionPande Indra PremanaNo ratings yet
- Rheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderDocument53 pagesRheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderPande Indra PremanaNo ratings yet
- Achondroplasia Emedicine DKKDocument29 pagesAchondroplasia Emedicine DKKPande Indra PremanaNo ratings yet
- Genetic Counseling and Prenatal DiagnosisDocument13 pagesGenetic Counseling and Prenatal DiagnosisPande Indra Premana100% (1)
- YAWAADocument10 pagesYAWAAZyrene CapulongNo ratings yet
- Hemorrahge Secondary To Multiple Stab WoundDocument26 pagesHemorrahge Secondary To Multiple Stab Wounddodong skyroseNo ratings yet
- Doctor ExhibitDocument110 pagesDoctor ExhibitKFORNo ratings yet
- Moderate Sedasi Di OKDocument10 pagesModerate Sedasi Di OKputu rusmiathiNo ratings yet
- Substance AbuseDocument87 pagesSubstance AbuseJayselle ArvieNo ratings yet
- GABA ReceptorDocument6 pagesGABA ReceptorAthena NocetoNo ratings yet
- Sleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsDocument50 pagesSleep Disorders in Children and Adolescents: Understanding Causes and Treatment OptionsCitra Sukri Sugesti100% (1)
- WithdrawalDocument102 pagesWithdrawalEga Candra FaurizaNo ratings yet
- Drug StudyDocument9 pagesDrug StudyVicenia BalloganNo ratings yet
- Mnemonic PharmaDocument13 pagesMnemonic Pharmamanoj kumarNo ratings yet
- Herbal Medicine and Anxiety DisorersDocument10 pagesHerbal Medicine and Anxiety DisorersSikander Ali BaigNo ratings yet
- PR 3Document23 pagesPR 3Jaylanie MabagaNo ratings yet
- Drug Study (Anesthesia)Document4 pagesDrug Study (Anesthesia)Jane Arian Berzabal100% (4)
- Mental Health2008Document4 pagesMental Health2008DonaJeanNo ratings yet
- Drug StudyDocument12 pagesDrug StudyMeraflor BahonsuaNo ratings yet
- Effects of Noise On Wildlife: BibliographyDocument70 pagesEffects of Noise On Wildlife: BibliographyAmelia TempletonNo ratings yet
- Care Management of The Agitation or Aggressiveness Crisis in Patients With TBI. Systematic Review of The Literature and Practice RecommendationsDocument10 pagesCare Management of The Agitation or Aggressiveness Crisis in Patients With TBI. Systematic Review of The Literature and Practice RecommendationsNers EducationNo ratings yet
- Psychopharmacology in Psychiatry: Neurotransmitter Pharmacology and Drug MechanismsDocument77 pagesPsychopharmacology in Psychiatry: Neurotransmitter Pharmacology and Drug MechanismschachaazkaNo ratings yet
- Pharmacologictreatment Fortemporomandibular Andtemporomandibularjoint DisordersDocument11 pagesPharmacologictreatment Fortemporomandibular Andtemporomandibularjoint DisordersDušanNo ratings yet
- Hospital FormularyDocument27 pagesHospital FormularyMarvin BernalesNo ratings yet
- 9aca PDFDocument11 pages9aca PDFJiayiNo ratings yet
- Neurotransmitters and Drugs ChartDocument6 pagesNeurotransmitters and Drugs ChartTammy Tam100% (5)
- Nurdiana. R PD-B/ 0810713031: Module TaskDocument10 pagesNurdiana. R PD-B/ 0810713031: Module TaskNurdiana RahmadaniNo ratings yet
- Substance AbuseDocument17 pagesSubstance AbuseRENEROSE TORRESNo ratings yet
- Alcohol and Anaesthesia - BJA Education - Oxford AcademicDocument14 pagesAlcohol and Anaesthesia - BJA Education - Oxford Academicayesha shaikNo ratings yet
- Generalized Anxiety Disorder A Case Study Submitted byDocument24 pagesGeneralized Anxiety Disorder A Case Study Submitted bySHARMAINE ANNE POLICIOS0% (1)
- SedatveDocument5 pagesSedatveUsman Ali AkbarNo ratings yet
- Brain Chemical ImbalanceDocument12 pagesBrain Chemical ImbalanceA. SerbanNo ratings yet
- PASSMED MRCP MCQs-PSYCHIATRYDocument33 pagesPASSMED MRCP MCQs-PSYCHIATRYStarlightNo ratings yet
- Chapter 2 - Neurobiologic Theories and PsychopharmacologyDocument11 pagesChapter 2 - Neurobiologic Theories and PsychopharmacologyCatia FernandesNo ratings yet