You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Filipino FamilyDocument11 pagesThe Filipino FamilyTiger Knee97% (37)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Laboratory Diagnosis of Viral InfectionDocument37 pagesLaboratory Diagnosis of Viral InfectionstudymedicNo ratings yet
- FrankensteinDocument24 pagesFrankensteinLisa WardNo ratings yet
- Pyrolysis ProjectDocument122 pagesPyrolysis ProjectSohel Bangi100% (1)
- Chich The ChickenDocument23 pagesChich The ChickenSil100% (4)
- The Arterial PulseDocument22 pagesThe Arterial PulsestudymedicNo ratings yet
- General Examination For CVSDocument29 pagesGeneral Examination For CVSstudymedic100% (1)
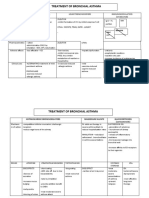
- Treatment of Bronchial AsthmaDocument3 pagesTreatment of Bronchial AsthmastudymedicNo ratings yet
- Pathology Practical Exam Study SheetDocument4 pagesPathology Practical Exam Study SheetstudymedicNo ratings yet
- History Taking in Pulmonary MedicineDocument14 pagesHistory Taking in Pulmonary MedicinestudymedicNo ratings yet
- First Line Agents (Essentials) in Treatment of TBDocument2 pagesFirst Line Agents (Essentials) in Treatment of TBstudymedicNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Jugular VeinsDocument13 pagesJugular VeinsstudymedicNo ratings yet
- Heart FailureDocument7 pagesHeart FailurestudymedicNo ratings yet
- Introduction To Platyhelminthes (Flukes)Document78 pagesIntroduction To Platyhelminthes (Flukes)studymedicNo ratings yet
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- Main Features of ParamyxovirusesDocument7 pagesMain Features of ParamyxovirusesstudymedicNo ratings yet
- Skills 2Document22 pagesSkills 2studymedicNo ratings yet
- Blood PressureDocument11 pagesBlood PressurestudymedicNo ratings yet
- Mumps VirusDocument15 pagesMumps Virusstudymedic0% (1)
- Rhino VirusesDocument20 pagesRhino VirusesstudymedicNo ratings yet
- Inspection and Palpation of The HeartDocument38 pagesInspection and Palpation of The Heartstudymedic100% (2)
- Orthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesDocument44 pagesOrthomyxoviruses Orthomyxoviruses Influenza Viruses Influenza VirusesstudymedicNo ratings yet
- Corona VirusesDocument42 pagesCorona VirusesstudymedicNo ratings yet
- Measles (Rubeola) VirusDocument16 pagesMeasles (Rubeola) Virusstudymedic100% (1)
- Adenoviruses AdenovirusesDocument25 pagesAdenoviruses AdenovirusesstudymedicNo ratings yet
- Practical Microbiology 2nd YearDocument33 pagesPractical Microbiology 2nd Yearstudymedic100% (1)
- Culture Media NoteDocument5 pagesCulture Media Notestudymedic100% (1)
- Vee 2003Document14 pagesVee 2003Syed faizan Ali zaidiNo ratings yet
- PPPoE Packet Format - HCNADocument6 pagesPPPoE Packet Format - HCNARobert Sanchez OchochoqueNo ratings yet
- Unit 5 Vocabulary Basic 1 Match 1-10 With A-J To Make Innovations and InventionsDocument6 pagesUnit 5 Vocabulary Basic 1 Match 1-10 With A-J To Make Innovations and InventionsCristina Garcia50% (2)
- DX DiagDocument42 pagesDX DiagVinvin PatrimonioNo ratings yet
- BH Tif03Document21 pagesBH Tif03Andres R. OlguinNo ratings yet
- A Comparison of Fuel Cell Testing Protocols PDFDocument7 pagesA Comparison of Fuel Cell Testing Protocols PDFDimitrios TsiplakidesNo ratings yet
- Learner's Activity Sheet: English (Quarter 4 - Week 5)Document5 pagesLearner's Activity Sheet: English (Quarter 4 - Week 5)Rufaidah AboNo ratings yet
- User Manual: C43J890DK C43J892DK C49J890DK C49J892DKDocument58 pagesUser Manual: C43J890DK C43J892DK C49J890DK C49J892DKGeorge FiruțăNo ratings yet
- Solution Proposal For SGF - BomDocument2 pagesSolution Proposal For SGF - BomABHISHEK ADHIKARYNo ratings yet
- Rigor Mortis and Lividity in Estimating Time of DeathDocument2 pagesRigor Mortis and Lividity in Estimating Time of DeathfunnyrokstarNo ratings yet
- Hireena Essay AnsDocument2 pagesHireena Essay AnsTasniiem ChandraaNo ratings yet
- Gizmotchy 3 Element Complete Assembly InstructionsDocument5 pagesGizmotchy 3 Element Complete Assembly InstructionsEuropaNo ratings yet
- Nodelman 1992Document8 pagesNodelman 1992Ana Luiza RochaNo ratings yet
- Newly Constructed Masculinity' in Mahesh Dattani's Dance Like A ManDocument4 pagesNewly Constructed Masculinity' in Mahesh Dattani's Dance Like A ManIJELS Research JournalNo ratings yet
- NVH PDFDocument3 pagesNVH PDFSubhendu BarisalNo ratings yet
- Day 2 TaskDocument4 pagesDay 2 TaskYaathriganNo ratings yet
- Application of Carbon-Polymer Based Composite Electrodes For Microbial Fuel CellsDocument26 pagesApplication of Carbon-Polymer Based Composite Electrodes For Microbial Fuel Cellsavinash jNo ratings yet
- Infineum Ilsa Gf-6 API SP e JasoDocument28 pagesInfineum Ilsa Gf-6 API SP e JasoDanielNo ratings yet
- Nurses Week Program InvitationDocument2 pagesNurses Week Program InvitationBenilda TuanoNo ratings yet
- Salt Analysis-Ferric ChlorideDocument3 pagesSalt Analysis-Ferric ChlorideVandana0% (1)
- IT Technician CVDocument3 pagesIT Technician CVRavi KumarNo ratings yet
- Estimating PSCC for Electrical InstallationsDocument2 pagesEstimating PSCC for Electrical InstallationsgmuitaNo ratings yet
- Schedule FinalDocument6 pagesSchedule FinalJamora ManilynNo ratings yet
- IELTS Writing Task 2/ IELTS EssayDocument2 pagesIELTS Writing Task 2/ IELTS EssayOlya HerasiyNo ratings yet
- Assurance Audit of Prepaid ExpendituresDocument7 pagesAssurance Audit of Prepaid ExpendituresRatna Dwi YulintinaNo ratings yet