You might also like
- Case Report OsteochondromaDocument43 pagesCase Report OsteochondromaFidesha Nurganiah SiregarNo ratings yet
- Osteoarthritis: Dr. C. C. VisserDocument85 pagesOsteoarthritis: Dr. C. C. VisserAhmad Fathira FitraNo ratings yet
- Case Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) HandDocument50 pagesCase Report: Osteoarthritis: Mutiara Riahna Sitepu 030.12.179 Pembimbing Dr. T. Nurrobi, SP - OT (K) Handmutiara sitepuNo ratings yet
- OA - Ahmad Aulia Rizaly - DR Andry Usman SpOTDocument34 pagesOA - Ahmad Aulia Rizaly - DR Andry Usman SpOTNur Syamsiah MNo ratings yet
- Assesment Rheumatoid ArthritisDocument39 pagesAssesment Rheumatoid ArthritisKlinik SakuramedicaNo ratings yet
- Ra and Osteoarthritis R IfDocument43 pagesRa and Osteoarthritis R IfsnfhanNo ratings yet
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- DR - Rieva Kuliah 7 November - 2018Document38 pagesDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
- Lec12 Sero Negative ArthritisDocument81 pagesLec12 Sero Negative ArthritistentenNo ratings yet
- Osteoarthritis 191016103144Document49 pagesOsteoarthritis 191016103144dr.abouzaid098No ratings yet
- Clinical and Applied Anatomy of The Lower Limb: Group Nine (9) Supervised By: Prof M.S Ajao Dr. IbrahimDocument118 pagesClinical and Applied Anatomy of The Lower Limb: Group Nine (9) Supervised By: Prof M.S Ajao Dr. IbrahimAlfanla Muh'd nasirNo ratings yet
- Common CasesDocument44 pagesCommon CasesRebecca WongNo ratings yet
- ImagesDocument430 pagesImagesSahan EpitawalaNo ratings yet
- Radiology Revision For MRCP IIDocument430 pagesRadiology Revision For MRCP IIMuntadher KareemNo ratings yet
- Pengayaan Koass Ortho - Update 5 VersionDocument122 pagesPengayaan Koass Ortho - Update 5 Versionanon_967171484No ratings yet
- Diapos y Lecturas UnidasDocument162 pagesDiapos y Lecturas UnidasOmar Benjamin Farroñan DiazNo ratings yet
- Disorders of The Foot and Leg ConfDocument304 pagesDisorders of The Foot and Leg ConfhaminatrafNo ratings yet
- N Amputation, Which Is The Removal of A Body Extremity. An Amputation Can Be Done Surgically or Occur As The Result of A Trauma Such As Being in An AccidentDocument8 pagesN Amputation, Which Is The Removal of A Body Extremity. An Amputation Can Be Done Surgically or Occur As The Result of A Trauma Such As Being in An AccidentMiloAndalesAntangJr.No ratings yet
- Femoral Neck FractureDocument37 pagesFemoral Neck FracturebikomuchtarNo ratings yet
- Managing Knee OsteoarthritisDocument32 pagesManaging Knee OsteoarthritisNurul Qalby AmiluddinNo ratings yet
- Departement of Orthopaedic and TraumatologyDocument89 pagesDepartement of Orthopaedic and TraumatologyMukhizalNo ratings yet
- Inflammatory Joint Diseases Handout-Admission ExamDocument11 pagesInflammatory Joint Diseases Handout-Admission ExamNona NadimNo ratings yet
- (MS1R) Common Representative Rheumatic DiseasesDocument6 pages(MS1R) Common Representative Rheumatic DiseasesYana DizonNo ratings yet
- 1-22 Osteoporosis & Hip PainDocument79 pages1-22 Osteoporosis & Hip PaintarikeopsNo ratings yet
- Anterior Knee Pain Syndrome ReferatDocument28 pagesAnterior Knee Pain Syndrome ReferatnurulNo ratings yet
- TB Spine OrthopedicsDocument34 pagesTB Spine OrthopedicsHafizah HoshniNo ratings yet
- Tuberculous ArthritisDocument34 pagesTuberculous ArthritisJeanette Callejas0% (1)
- Osteoarthritis and GoutDocument69 pagesOsteoarthritis and Goutadamu mohammadNo ratings yet
- Regional pathologies and evaluation: Tendon – Muscle – Cartilage and NerveDocument18 pagesRegional pathologies and evaluation: Tendon – Muscle – Cartilage and NerveAly MssreNo ratings yet
- Osteo Arthritis and Inflammatory Arthritis: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaDocument45 pagesOsteo Arthritis and Inflammatory Arthritis: DR - Yanto Budiman. SP - Rad, M.Kes Bagian Radiologi FK/RS. Atma JayaMira FindoroNo ratings yet
- Surgical Treatment of Neglected Malunion of Shaft Femur: Case ReportDocument13 pagesSurgical Treatment of Neglected Malunion of Shaft Femur: Case ReportNando OktariNo ratings yet
- MSK Study Schedule 2Document12 pagesMSK Study Schedule 2Aashish GiriNo ratings yet
- Rheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresDocument25 pagesRheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresNinaNo ratings yet
- ARTHRITIS LectureDocument5 pagesARTHRITIS LectureMacDonald KarikariNo ratings yet
- AIR FlimDocument69 pagesAIR FlimRapid MedicineNo ratings yet
- Muh. Ismail Pratama A. Tenri Luwu MutmainnahDocument34 pagesMuh. Ismail Pratama A. Tenri Luwu MutmainnahNurul Qalby AmiluddinNo ratings yet
- Disorders of Skeletal SystemDocument24 pagesDisorders of Skeletal SystemAleksa JovanovicNo ratings yet
- Myth-Busting Facts About OsteoarthritisDocument17 pagesMyth-Busting Facts About OsteoarthritisMuskan khaziNo ratings yet
- Myositis Ossificans: Causes, Symptoms and TreatmentDocument20 pagesMyositis Ossificans: Causes, Symptoms and TreatmentsarathNo ratings yet
- Advisor: DR - Padlan DR - Luthf Supervisor: Dr. Notinas Horas, M.Kes, SP - OT Orthopaedic and Traumatology DepartmentDocument34 pagesAdvisor: DR - Padlan DR - Luthf Supervisor: Dr. Notinas Horas, M.Kes, SP - OT Orthopaedic and Traumatology DepartmentroserosannaNo ratings yet
- Osteonecrosis: Jamal Abu Helal Orthopedic Consultant EGHDocument50 pagesOsteonecrosis: Jamal Abu Helal Orthopedic Consultant EGHlina jamalNo ratings yet
- Benign Joint Hypermobility SyndromeDocument23 pagesBenign Joint Hypermobility SyndromeAli TawbeNo ratings yet
- Arthritis 180325095830 PDFDocument77 pagesArthritis 180325095830 PDFHesoca HuxNo ratings yet
- OsteoarthritisDocument40 pagesOsteoarthritiskylieverNo ratings yet
- Osteoarthritis: Heberden's NodesDocument4 pagesOsteoarthritis: Heberden's NodesAmalNo ratings yet
- Closed Fraktur Distal Tibia FibulaDocument27 pagesClosed Fraktur Distal Tibia FibulaAnggita Efipania Silambi'No ratings yet
- ARTHRITIS TB KNEE HIP BPTDocument84 pagesARTHRITIS TB KNEE HIP BPTMiso100% (1)
- SPINAL CORD INJURY OVERVIEWDocument59 pagesSPINAL CORD INJURY OVERVIEWfazliahNo ratings yet
- Medscape Knee OCDDocument16 pagesMedscape Knee OCDDita Ambarsari SyafruddinNo ratings yet
- 06-Dr. Bajammal Hip Disorders 2017Document48 pages06-Dr. Bajammal Hip Disorders 2017MuathNo ratings yet
- Oa Ar GoutDocument18 pagesOa Ar GoutnerdwaldoNo ratings yet
- Osteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Document64 pagesOsteoarthritis: (Degenerative Arthritis/osteoarthrosis/hypertrophic Arthritis)Linda SugiartoNo ratings yet
- Presentasi Kasus Batu Pyelum KananDocument46 pagesPresentasi Kasus Batu Pyelum KananAdrian Himawan SinggihNo ratings yet
- Giant Cell Tumor: MUH - YUSUF M C11111 893 NURHIDAYAH C11111 120 Yoriche Tallamma C11111 293 Andi Nirmawati. Ar C11112 063Document34 pagesGiant Cell Tumor: MUH - YUSUF M C11111 893 NURHIDAYAH C11111 120 Yoriche Tallamma C11111 293 Andi Nirmawati. Ar C11112 063AndinNo ratings yet
- Update A1 OsceDocument120 pagesUpdate A1 OsceIndra SetyaNo ratings yet
- Arthritis: Prepared By: Salini D/O Vasudevan Supervisor: DR JaneDocument73 pagesArthritis: Prepared By: Salini D/O Vasudevan Supervisor: DR Janeumanantini06No ratings yet
- What's Your Call?: Clinical Vistas BriefsDocument2 pagesWhat's Your Call?: Clinical Vistas BriefsHeri Hrisikesa WjgNo ratings yet
- Nursing Management of A Patient With Femoral Neck FractureDocument12 pagesNursing Management of A Patient With Femoral Neck Fracturedanni L100% (6)
- Lembar Triage PDFDocument1 pageLembar Triage PDFEliana MuisNo ratings yet
- Diet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Document22 pagesDiet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Eliana MuisNo ratings yet
- Lembar TriageDocument1 pageLembar TriageEliana MuisNo ratings yet
- PleurodesisDocument30 pagesPleurodesisEliana Muis100% (1)
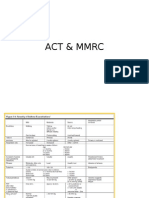
- ACT & MMRC Assessment ToolsDocument9 pagesACT & MMRC Assessment ToolsEliana MuisNo ratings yet
- Diet July07Document25 pagesDiet July07Eliana MuisNo ratings yet
- DM Lecture FDocument98 pagesDM Lecture FEliana MuisNo ratings yet
- Diabetes Medications: An Overview: Eric L. Johnson, M.DDocument62 pagesDiabetes Medications: An Overview: Eric L. Johnson, M.DEliana MuisNo ratings yet
- Sarana PrasaranaDocument5 pagesSarana PrasaranaEliana MuisNo ratings yet
- Review Paper MDR-TB PDFDocument12 pagesReview Paper MDR-TB PDFEliana MuisNo ratings yet
- Diabetes 101: A Brief Overview of Diabetes and The American Diabetes AssociationDocument32 pagesDiabetes 101: A Brief Overview of Diabetes and The American Diabetes AssociationEliana MuisNo ratings yet
- Insulin TherapyDocument23 pagesInsulin TherapyEliana MuisNo ratings yet
- Spirometry and DiabetesDocument2 pagesSpirometry and DiabetesEliana MuisNo ratings yet
- Pub Tb-Hivguide Eng WebDocument0 pagesPub Tb-Hivguide Eng WebEliana MuisNo ratings yet
- Ethics For Coughing SmallDocument1 pageEthics For Coughing SmallEliana MuisNo ratings yet
- Cancerization: Evidence and Clinical Implications A Genetic Explanation of Slaughter's Concept of FieldDocument5 pagesCancerization: Evidence and Clinical Implications A Genetic Explanation of Slaughter's Concept of FieldEliana MuisNo ratings yet
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyEliana MuisNo ratings yet
- JCO 2011 Morris 739 46Document8 pagesJCO 2011 Morris 739 46Eliana MuisNo ratings yet
- DEPKES RI 2011 Pedoman Penanggulangan TB Di Indonesia PDFDocument59 pagesDEPKES RI 2011 Pedoman Penanggulangan TB Di Indonesia PDFMartin Susanto, MD100% (9)
- Smoking CessationDocument4 pagesSmoking CessationEliana MuisNo ratings yet
- Int STD TB Care 2009Document84 pagesInt STD TB Care 2009paulmusilaNo ratings yet
- Guidelines TBC TerbaruDocument160 pagesGuidelines TBC TerbaruSutoto MoeljadiNo ratings yet
- Tuberculosis2012 - International Congress - Scientific ProgramDocument9 pagesTuberculosis2012 - International Congress - Scientific ProgramEliana MuisNo ratings yet
- Eng 3 Q1Wk11Document7 pagesEng 3 Q1Wk11CRISTILE ANN GESMAN100% (1)
- I) Underline The Correct FormDocument6 pagesI) Underline The Correct FormSơn VũNo ratings yet
- Alfred Jensen Paintings and Works On PaperDocument88 pagesAlfred Jensen Paintings and Works On PaperSabri Gutierrez100% (1)
- Management AccountingDocument42 pagesManagement AccountingaamritaaNo ratings yet
- Long-Run and Short-Run Concerns: Growth, Productivity, Unemployment, and in AtionDocument34 pagesLong-Run and Short-Run Concerns: Growth, Productivity, Unemployment, and in AtionYunita AngelicaNo ratings yet
- Answer KeyDocument5 pagesAnswer KeyGurjot SinghNo ratings yet
- XXX Marketing StrategyDocument9 pagesXXX Marketing StrategyJoel MitchellNo ratings yet
- RAD Studio LiveBindings GuideDocument63 pagesRAD Studio LiveBindings Guidewolfie002No ratings yet
- 6D125-2 Engine (PC450-6) Shop Manual (SEBM006410)Document366 pages6D125-2 Engine (PC450-6) Shop Manual (SEBM006410)cuthuongtho92% (51)
- Jacqueline Thompson: Marketing ManagerDocument1 pageJacqueline Thompson: Marketing ManagerAndreia LealNo ratings yet
- GE Nine Cell MatrixDocument1 pageGE Nine Cell MatrixSunil Kakkar100% (4)
- SANLAKAS v. ReyesDocument2 pagesSANLAKAS v. Reyesglecie_co12No ratings yet
- A Town Planning Board Must Decide How To Deal WithDocument1 pageA Town Planning Board Must Decide How To Deal Withtrilocksp SinghNo ratings yet
- Intelligent Traffic Management Using SDNDocument5 pagesIntelligent Traffic Management Using SDNEngr XsadNo ratings yet
- Camilleri January 24 2019 BOE StatementDocument3 pagesCamilleri January 24 2019 BOE StatementHelen BennettNo ratings yet
- Mismatch Defect in ERW Steel Tubes: September 2014Document5 pagesMismatch Defect in ERW Steel Tubes: September 2014Riza KhanNo ratings yet
- Editing ScriptsDocument17 pagesEditing ScriptssisyololoNo ratings yet
- ECLYPSE™ Connected Terminal Unit Controller: Product DescriptionDocument16 pagesECLYPSE™ Connected Terminal Unit Controller: Product DescriptionandyvtranNo ratings yet
- Intro to Project Management FundamentalsDocument54 pagesIntro to Project Management FundamentalsDiriba MokononNo ratings yet
- 7 FacetsDocument2 pages7 Facetsdeanyangg25No ratings yet
- Ertyuikjrewdefthyjhertyujkreytyjthm VCDocument2 pagesErtyuikjrewdefthyjhertyujkreytyjthm VCCedrick Jasper SanglapNo ratings yet
- "Who Can Shave An Egg?" - Beckett, Mallarmé, and Foreign Tongues.Document29 pages"Who Can Shave An Egg?" - Beckett, Mallarmé, and Foreign Tongues.Aimee HarrisNo ratings yet
- Consumer Behavior Factors in Nike's "Find Your GreatnessDocument3 pagesConsumer Behavior Factors in Nike's "Find Your GreatnessReynaldo Budi RahardjaNo ratings yet
- Chevron SealDocument7 pagesChevron Sealwenny_tpdNo ratings yet
- Oral-COm WK 1Document3 pagesOral-COm WK 1bernadette domoloanNo ratings yet
- Bitwise Operations in CDocument18 pagesBitwise Operations in CPriyam ChowdhuryNo ratings yet
- Curriculum Vitea P.G.C.MDocument3 pagesCurriculum Vitea P.G.C.MMushtaq AhmadNo ratings yet
- Criminal Justice SytemDocument14 pagesCriminal Justice SytemMarc Lester100% (1)
- RAICES LawsuitDocument25 pagesRAICES LawsuitJohn MoritzNo ratings yet
- Prepared By: Eva Marie Demple Soliman Noted By: DR. MARILOU H. MELLA - DeanDocument27 pagesPrepared By: Eva Marie Demple Soliman Noted By: DR. MARILOU H. MELLA - DeanJonadel GeronaNo ratings yet