You might also like
- Uterine ProlapseDocument3 pagesUterine ProlapsefrankyNo ratings yet
- Overview Antenatal CareDocument54 pagesOverview Antenatal CareRizky Dwidya AmirtasariNo ratings yet
- Ovarian TorsionDocument48 pagesOvarian Torsionmaria ilyasNo ratings yet
- Intrauterine Contraception: Copper T 380A (Paragard®) Levonorgestrel-Releasing Intrauterine System (Mirena®)Document16 pagesIntrauterine Contraception: Copper T 380A (Paragard®) Levonorgestrel-Releasing Intrauterine System (Mirena®)Fia Delfia AdventyNo ratings yet
- Male InfertilityDocument63 pagesMale InfertilitySuhaila SabanNo ratings yet
- Antenatal CareDocument29 pagesAntenatal CareAsti Yuliadha100% (3)
- Case Report on Severe PreeclampsiaDocument98 pagesCase Report on Severe Preeclampsianovika100% (1)
- MVA Manual Vacuum Aspiration Abortion Procedure GuideDocument23 pagesMVA Manual Vacuum Aspiration Abortion Procedure GuideAjay JadejaNo ratings yet
- Relationship between maternal knowledge level and pushing technique on the incidence of perineal ruptureDocument47 pagesRelationship between maternal knowledge level and pushing technique on the incidence of perineal ruptureayu fitria0% (1)
- Urinary IncontinenceDocument66 pagesUrinary Incontinencedr_asaleh100% (1)
- Diagnosing Undisturbed vs Disturbed Tubal Ectopic PregnanciesDocument1 pageDiagnosing Undisturbed vs Disturbed Tubal Ectopic PregnancieskukadiyaNo ratings yet
- Menopause & HRT: Effects, Management and ControversiesDocument27 pagesMenopause & HRT: Effects, Management and ControversiesMajed AlhuzaliNo ratings yet
- Obg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementDocument81 pagesObg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementElakkiyaanu64 Elakkiyaanu64No ratings yet
- Safe Motherhood PDFDocument13 pagesSafe Motherhood PDFcarissa rhezaNo ratings yet
- FK UNS OBGIN USG 1i. Skrining Anomali Trimester Dua ISUOG Guidelines JJE 20120609Document66 pagesFK UNS OBGIN USG 1i. Skrining Anomali Trimester Dua ISUOG Guidelines JJE 20120609Judi Januadi Endjun, MD, ObsGyn100% (1)
- Intrauterine Growth RestrictionDocument3 pagesIntrauterine Growth RestrictionShofiKhaqulIlmyNo ratings yet
- TORCH in PregnancyDocument63 pagesTORCH in PregnancySaRah AmiThia SaRi BuLanNo ratings yet
- Dr. Hardjono Purwadhi SpOG. Gynecologic Cancer Distribution : IndonesiaDocument47 pagesDr. Hardjono Purwadhi SpOG. Gynecologic Cancer Distribution : IndonesiaMuhammad SidiqNo ratings yet
- Keehbauch Menopause HRT 4.2.16 SCDocument55 pagesKeehbauch Menopause HRT 4.2.16 SCMuhammad AzkaNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument54 pagesInduction of Labor With Oxytocin - UpToDateJhoseline CamposNo ratings yet
- Recurrent MiscarriageDocument6 pagesRecurrent MiscarriageuzmajbnNo ratings yet
- KontrasepsiDocument30 pagesKontrasepsiElsaIsabelSilaenNo ratings yet
- Risk of Postpartum Infections (39Document29 pagesRisk of Postpartum Infections (39gerryneutron100% (1)
- Hiperemesis GravidarumDocument12 pagesHiperemesis GravidarumDayita ApritutiNo ratings yet
- IUFDDocument29 pagesIUFDfasyanneshaNo ratings yet
- Screening and Diagnosis of High-Risk PregnancyDocument44 pagesScreening and Diagnosis of High-Risk PregnancyKavipriyaNo ratings yet
- Amenore PrimerDocument40 pagesAmenore PrimerMaksum Pandelima0% (1)
- Occiput Posterior Position Diagnosis VagDocument19 pagesOcciput Posterior Position Diagnosis VagMutianaUmminyaKhanzaNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Intrauterine Growth RestrictionDocument7 pagesIntrauterine Growth RestrictionNurfazlinaNo ratings yet
- Edited Maternal ProcedureDocument45 pagesEdited Maternal ProcedureClare Alcober100% (1)
- Advancement in Partograph WHO's Labor Care GuideDocument7 pagesAdvancement in Partograph WHO's Labor Care GuideSujan ThapaNo ratings yet
- Development of Uterus and Congenital Anomalies: Done By: Jabir AL Araimi ID# 0333145Document21 pagesDevelopment of Uterus and Congenital Anomalies: Done By: Jabir AL Araimi ID# 0333145jabirNo ratings yet
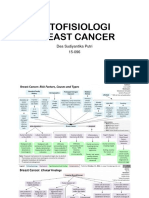
- Pathophysiology of Breast CancerDocument5 pagesPathophysiology of Breast CancerDichaNo ratings yet
- Ovarian Torsion PDFDocument35 pagesOvarian Torsion PDFitshijabi vlogsNo ratings yet
- CTG Classification PDFDocument1 pageCTG Classification PDFAkhmad Ikhsan Prafita PutraNo ratings yet
- Infertilityseminarppt 190718134710Document77 pagesInfertilityseminarppt 190718134710subiNo ratings yet
- Acute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalDocument73 pagesAcute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalIgnatov OanaNo ratings yet
- Breast EngorgementDocument14 pagesBreast EngorgementIvan KurniadiNo ratings yet
- MRKH Sundrome PPTDocument37 pagesMRKH Sundrome PPTleenarobin100% (2)
- Case Report On Fibroid UterusDocument4 pagesCase Report On Fibroid UterusInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- EndometritisDocument21 pagesEndometritisRoshni SunarNo ratings yet
- Ultrasound Diagnosis of Early Pregnancy LossDocument18 pagesUltrasound Diagnosis of Early Pregnancy LossxxdrivexxNo ratings yet
- Vaginal Discharge Causes and TreatmentsDocument14 pagesVaginal Discharge Causes and TreatmentsMsharaniaNo ratings yet
- Septic AbortionDocument15 pagesSeptic Abortionapi-3705046No ratings yet
- Ovarian Torsion After Ovarian Hyperstimulation SyndromeDocument2 pagesOvarian Torsion After Ovarian Hyperstimulation SyndromeasclepiuspdfsNo ratings yet
- Jadwal Pit (Fetomaternal Room)Document3 pagesJadwal Pit (Fetomaternal Room)Dwi Adi NugrohoNo ratings yet
- Ovarian Torsion: Angie Child, Harvard Medical School IV Gillian Lieberman, MDDocument27 pagesOvarian Torsion: Angie Child, Harvard Medical School IV Gillian Lieberman, MDNishchay TripathiNo ratings yet
- Case Report HEGDocument16 pagesCase Report HEGcitraNo ratings yet
- Understanding HIV and HAART ManagementDocument33 pagesUnderstanding HIV and HAART ManagementWill CheahNo ratings yet
- Case Study On Fibroid UterusDocument68 pagesCase Study On Fibroid UterusSeenha DewanNo ratings yet
- Postterm Pregnancy - UpToDateDocument17 pagesPostterm Pregnancy - UpToDateJosé Abraham Amaya DuarteNo ratings yet
- Referat: Abnormal Uerine Bleeding (AUB)Document28 pagesReferat: Abnormal Uerine Bleeding (AUB)Norbertus MacekaNo ratings yet
- Skor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermDocument9 pagesSkor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermMuhammad KhoiruddinNo ratings yet
- Dr. Kruvilla - Hyperthyroidism in PregnancyDocument38 pagesDr. Kruvilla - Hyperthyroidism in PregnancyjarvantaraNo ratings yet
- Uterine Fibroid Treatment OptionsDocument20 pagesUterine Fibroid Treatment OptionscopperNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Intrauterine Device (IUD)Document46 pagesIntrauterine Device (IUD)semegn0936No ratings yet
- Etiology: Abortion Is Used To Indicate The Release of The Results of Conception Before The Fetus Can LiveDocument6 pagesEtiology: Abortion Is Used To Indicate The Release of The Results of Conception Before The Fetus Can LiveRico IrawanNo ratings yet
- Management of Intrauterine Fetal Demise: CCHS Grand Rounds June 2018Document32 pagesManagement of Intrauterine Fetal Demise: CCHS Grand Rounds June 2018AlexandruBabianNo ratings yet
- Evidence For Camel-to-Human Transmission of MERS CoronavirusDocument7 pagesEvidence For Camel-to-Human Transmission of MERS CoronavirusTantix's SeororoNo ratings yet
- The European Stroke Organisation Guidelines 2014Document2 pagesThe European Stroke Organisation Guidelines 2014Anonymous omvOqGHX2FNo ratings yet
- The European Stroke Organisation Guidelines 2014Document2 pagesThe European Stroke Organisation Guidelines 2014Anonymous omvOqGHX2FNo ratings yet
- SSC Implementation GuideDocument71 pagesSSC Implementation GuideciptaNo ratings yet
- Pterygium Prevalence and Characteristics in IndonesiaDocument6 pagesPterygium Prevalence and Characteristics in IndonesiaAnonymous omvOqGHX2FNo ratings yet
- ESC Universal Definition of MI (2007)Document14 pagesESC Universal Definition of MI (2007)Anonymous omvOqGHX2FNo ratings yet
- Iron Deficiency Anemia WHODocument10 pagesIron Deficiency Anemia WHOAnonymous omvOqGHX2FNo ratings yet
- Iron Deficiency AnaemiaDocument132 pagesIron Deficiency AnaemiaHectorNo ratings yet
- Book 2Document5 pagesBook 2Anonymous omvOqGHX2FNo ratings yet
- GiftasupDocument50 pagesGiftasupFizza SiddiquiNo ratings yet
- Sinonasal ReviewDocument18 pagesSinonasal ReviewZsa Zsa MarananiNo ratings yet
- BurnsDocument23 pagesBurnsAnonymous omvOqGHX2FNo ratings yet
- Penyakit Inf Saluran Pencernaan PDFDocument9 pagesPenyakit Inf Saluran Pencernaan PDFAde PermanaNo ratings yet
- Immuno TherapyDocument12 pagesImmuno TherapyAnonymous omvOqGHX2FNo ratings yet
- Class12th HUMAN-REPRODUCTION PDFDocument29 pagesClass12th HUMAN-REPRODUCTION PDFShubhang CharantimathNo ratings yet
- Chapter 9Document16 pagesChapter 9anil.gelra5140No ratings yet
- Resumenes Congreso 2013Document263 pagesResumenes Congreso 2013Gloria Jara MNo ratings yet
- Sexing Day Old ChicksDocument4 pagesSexing Day Old ChicksrabatitatNo ratings yet
- NCERT Solutions For Class 12 Biology Chapter 1-Reproduction in OrganismsDocument11 pagesNCERT Solutions For Class 12 Biology Chapter 1-Reproduction in OrganismsRajveer SinghNo ratings yet
- Worksheet 16.2: Self-And Cross-PollinationDocument2 pagesWorksheet 16.2: Self-And Cross-PollinationShahed Bulbul PaponNo ratings yet
- Mitosis Meiosis NotesDocument7 pagesMitosis Meiosis NotesSophia Cook100% (1)
- Family PlanningDocument10 pagesFamily Planningdalvin20207967No ratings yet
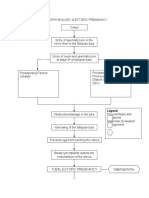
- PATHOPHYSIOLOGY of ECTOPIC PREGNANCYDocument2 pagesPATHOPHYSIOLOGY of ECTOPIC PREGNANCYrye100% (1)
- Chapter 38 Animal DevelopmentDocument77 pagesChapter 38 Animal Developmentmaria banunaekNo ratings yet
- Expectations as an Egg DonorDocument2 pagesExpectations as an Egg DonorNini LekishviliNo ratings yet
- Reproductive System With HighlightsDocument150 pagesReproductive System With HighlightsReinand Joseff ServanoNo ratings yet
- Pengaruh Lama Penyimpanan DAN Warna Kerabang Terhadap Kualitas Internal Telur Ayam RASDocument7 pagesPengaruh Lama Penyimpanan DAN Warna Kerabang Terhadap Kualitas Internal Telur Ayam RASDanuartaNo ratings yet
- General-Biology-2-PRELIM-EXAM - MAGBANUA STEM 11BDocument4 pagesGeneral-Biology-2-PRELIM-EXAM - MAGBANUA STEM 11BSophia MagbanuaNo ratings yet
- Teaching and Learning Module KSSR (Semakan 2017) Science Year 6Document116 pagesTeaching and Learning Module KSSR (Semakan 2017) Science Year 6LING KUOK LIMNo ratings yet
- Recent Advances in The Application of Plant Tissue Culture in DieffenbachiaDocument10 pagesRecent Advances in The Application of Plant Tissue Culture in DieffenbachiaaguilaquecaeNo ratings yet
- 9700 m16 QP 42 PDFDocument28 pages9700 m16 QP 42 PDFAtef Ibrahim KhalifaNo ratings yet
- Modeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsDocument22 pagesModeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsKerin ArdyNo ratings yet
- The Miracle of Life, Images of Gestation of Baby in The Womb, in Utero Photos of An Embryo With Development From Conception To Birth.Document17 pagesThe Miracle of Life, Images of Gestation of Baby in The Womb, in Utero Photos of An Embryo With Development From Conception To Birth.Lily of the ValleysNo ratings yet
- The Organs of The Male Reproductive System Are Specialized For The Following FunctionsDocument3 pagesThe Organs of The Male Reproductive System Are Specialized For The Following FunctionsGabrielaNo ratings yet
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton86% (14)
- 10th Biology Mcqs NotesDocument31 pages10th Biology Mcqs Notessupersaad987No ratings yet
- Lesson 1 Stallion Management PowerpointDocument25 pagesLesson 1 Stallion Management PowerpointelblazerNo ratings yet
- Campbell 2020 1Document25 pagesCampbell 2020 1wonderwellNo ratings yet
- MCN LectureDocument8 pagesMCN LectureEmily BernatNo ratings yet
- Al-Khair Higher Secondary School.: ObjectiveDocument2 pagesAl-Khair Higher Secondary School.: ObjectiveTariq MuneerNo ratings yet
- Population EcologyDocument21 pagesPopulation EcologyJeemCarloFagelaPulaNo ratings yet
- 61 Irregular Verbs Pink and PurpleDocument18 pages61 Irregular Verbs Pink and PurpleRebeca HR SKNo ratings yet
- Biology II: Continuity of Life Macromolecules and MicromoleculesDocument23 pagesBiology II: Continuity of Life Macromolecules and MicromoleculesLester Randy RubintinusNo ratings yet
- Sexual Reproduction in Flowering Plants QuestionsDocument11 pagesSexual Reproduction in Flowering Plants QuestionsAjayNo ratings yet