You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Pain Physiology Chapter Explains Nociception and HyperalgesiaDocument20 pagesPain Physiology Chapter Explains Nociception and HyperalgesiaDiana TiganucNo ratings yet
- q1 l1 Energy SystemDocument30 pagesq1 l1 Energy SystemJaysonMananquilLabsan100% (1)
- Cardiology in The ElderlyDocument67 pagesCardiology in The ElderlyDiana TiganucNo ratings yet
- Cardiovascular Agents ReviewerDocument18 pagesCardiovascular Agents ReviewerJoycel CeñidozaNo ratings yet
- Conjuctivitis: 1. BacterialDocument11 pagesConjuctivitis: 1. BacterialDiana TiganucNo ratings yet
- Biological Psychology Kalat 12th Edition Solutions ManualDocument12 pagesBiological Psychology Kalat 12th Edition Solutions ManualJames Pennington100% (35)
- DR Podcast Scripts For The Final FRCADocument2 pagesDR Podcast Scripts For The Final FRCADiana Tiganuc50% (2)
- Easy Way To Learn ABGsDocument13 pagesEasy Way To Learn ABGsMunaim TahirNo ratings yet
- Ethier Introductory Bio Mechanics From Cells To Organisms Cambridge 2007Document545 pagesEthier Introductory Bio Mechanics From Cells To Organisms Cambridge 2007hoplala100% (1)
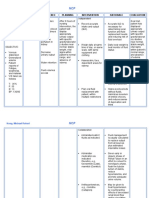
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMr. whiteNo ratings yet
- DX Intracranial Pressure PDFDocument8 pagesDX Intracranial Pressure PDFSherree HayesNo ratings yet
- V2 Compendiu de Specialitati Medico-Chirurgicale (Rezidentiat - V.stoica Si V.scripcariu)Document402 pagesV2 Compendiu de Specialitati Medico-Chirurgicale (Rezidentiat - V.stoica Si V.scripcariu)andrei089191% (11)
- Recommended Reading List For EDAIC PDFDocument5 pagesRecommended Reading List For EDAIC PDFDiana TiganucNo ratings yet
- Ghid Resuscitare 2015Document53 pagesGhid Resuscitare 2015Diana TiganucNo ratings yet
- End Tidal CoDocument79 pagesEnd Tidal CoDiana Tiganuc100% (1)
- Travel List German 1Document284 pagesTravel List German 1Neacsu AndreiNo ratings yet
- VAP ProphylaxisDocument50 pagesVAP ProphylaxisDiana TiganucNo ratings yet
- Guidelines Perioperative Cardiac Care FTDocument44 pagesGuidelines Perioperative Cardiac Care FTNaren ReddyNo ratings yet
- End Tidal CoDocument79 pagesEnd Tidal CoDiana Tiganuc100% (1)
- ''Sangrado Perioperatorio Severo GuiaDocument113 pages''Sangrado Perioperatorio Severo GuiaHECTOR ESTRADANo ratings yet
- Hypertension in Geriatric PopulationDocument52 pagesHypertension in Geriatric PopulationDiana TiganucNo ratings yet
- Delirium - GeriatrieDocument61 pagesDelirium - GeriatrieDiana TiganucNo ratings yet
- Insomnia PDFDocument33 pagesInsomnia PDFElena IonesiNo ratings yet
- Vector Basics of 12 Lead ECG SDocument17 pagesVector Basics of 12 Lead ECG SDiana TiganucNo ratings yet
- Adult Vaccine ScheduleDocument3 pagesAdult Vaccine ScheduleAnonymous gjYDftNo ratings yet
- Acute Coronary SyndromesDocument28 pagesAcute Coronary SyndromesDiana TiganucNo ratings yet
- Adult Vaccine ScheduleDocument3 pagesAdult Vaccine ScheduleAnonymous gjYDftNo ratings yet
- Evaluare Ecocardiografica A Functiei Diastolice A VsDocument6 pagesEvaluare Ecocardiografica A Functiei Diastolice A VsDiana TiganucNo ratings yet
- Bleeding in First Trimester - Miscarriage, Non-Obstetrical ReasonsDocument23 pagesBleeding in First Trimester - Miscarriage, Non-Obstetrical ReasonsDiana TiganucNo ratings yet
- Management of Shock in ChildrenDocument26 pagesManagement of Shock in ChildrenkarinakerenNo ratings yet
- Lymphatic SystemDocument29 pagesLymphatic SystemlecturioNo ratings yet
- WBCs Chap 2Document119 pagesWBCs Chap 2Hoor ul Ain RamzanNo ratings yet
- Risks & Benefits of Blood TransfusionDocument34 pagesRisks & Benefits of Blood TransfusionBryand KostaNo ratings yet
- Drug Study LabetalolDocument2 pagesDrug Study LabetalolJanzelvine Lee MontenegroNo ratings yet
- Electrolyte and Fluid Imbalances ChartDocument8 pagesElectrolyte and Fluid Imbalances ChartChrizley Shawn DeroniaNo ratings yet
- Stool HomeoDocument35 pagesStool HomeoBabli Lovely NickyNo ratings yet
- Blood - WikipediaDocument106 pagesBlood - WikipediaZoha AliNo ratings yet
- Ch03 Questions Answer KeyDocument18 pagesCh03 Questions Answer KeyMichaelNo ratings yet
- Modul 1. Patofisiologi ACSDocument24 pagesModul 1. Patofisiologi ACSFadhilAfifNo ratings yet
- Yang Et Al, 2020 - O Papel Do BDNF Na Plasticidade Neural Na DepressãoDocument12 pagesYang Et Al, 2020 - O Papel Do BDNF Na Plasticidade Neural Na Depressãoprofessor do valeNo ratings yet
- N 682 Applied Physiology For Nurse Anesthesia IIDocument7 pagesN 682 Applied Physiology For Nurse Anesthesia IIapi-267840127No ratings yet
- Metanalisis Elevacion Pasiva de MMIIDocument11 pagesMetanalisis Elevacion Pasiva de MMIImayraNo ratings yet
- DR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalDocument53 pagesDR Sujata: Professor Dept - of Anaesthesiology &critical Care Ucms & GTB HospitalMiniNo ratings yet
- Grade 11 HypertemiaDocument25 pagesGrade 11 Hypertemiarom kero0% (1)
- QuestionsDocument4 pagesQuestionsProduktemeuljeNo ratings yet
- HUBS191 Endocrine SystemDocument1 pageHUBS191 Endocrine SystemLee Jia QingNo ratings yet
- Vascular Study GuideDocument2 pagesVascular Study GuideApril Danielle TeschNo ratings yet
- High Altitude Deep Sea Diving & ExcerciseDocument18 pagesHigh Altitude Deep Sea Diving & ExcercisegiannidietNo ratings yet
- Physical ExamDocument25 pagesPhysical Examlady birdNo ratings yet
- Muscle Tissue LabDocument2 pagesMuscle Tissue LabAce MozcareNo ratings yet
- Essentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewDocument15 pagesEssentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewMariana MadridNo ratings yet
- Reading as a Physiological ProcessDocument2 pagesReading as a Physiological ProcessJee DeeNo ratings yet
- Nursing Care Plan for Fluid Volume DeficitDocument2 pagesNursing Care Plan for Fluid Volume DeficitJohnrick VenturaNo ratings yet